
記住我






The survey included 20 respondents, each representing a different hospital. The characteristics of the respondents are as follows: 17 were males (85%), 3 were females, and their ages ranged from 21 to 40 years old. All respondents held a college or university degree and worked as Biomedical engineer/Technician in their roles for 1–9 years.
3.1 General information about the facilitiesAmongst the 20 hospitals assessed, there are 19 public hospitals and one Non-governmental Hospital (NGO). Tertiary- level hospitals account for 40%, secondary-level hospitals for 20%, and primary hospitals for the remaining 40% The inclusion of different levels of hospitals in the assessment allowed for a comprehensive understanding of the healthcare landscape, considering their diverse capabilities, services, and resources available.
In terms of water sources, 13 hospitals (65%) primarily use piped water, while a mix of tanker water and open well water is common; three hospitals (15%) rely solely on tanker water; and the remaining hospitals (15%) use various water sources, except for one hospital (5%) that relies on open well water. Regarding communication infrastructure, 16 hospitals (80%) have operational landline telephones, while three hospitals do not (15%). One (5%) respondent was unsure about the type of communication system used by their hospital. Additionally, 15 hospitals (75%) have functional mobile phones, while four hospitals do not. None of the hospitals have short-wave radio wave facilities. Approximately, 90% of the facilities have at least one operational computer for staff use. Finally, 75% of the hospitals have a working internet connection, and all the hospitals assessed have at least one ambulance available.
3.2 Electrical access and safetyThe assessment found that all hospitals had electricity access: eight relied on central power, two on generators, and ten had both. In the previous month, 11 hospitals experienced over 10 power disruptions, two had 7–9 disruptions, four had 4–6, and three faced 1–3 disruptions.
For electrical safety, ten hospitals used grounding, three had both grounding and isolation transformers, and two relied only on isolation transformers. No hospitals had equipotential grounding devices, and five hospitals were unsure of their safety systems. Electrical safety ratings varied: four respondents rated it as “Very Poor,” eight as “Poor,” seven as “Acceptable,” and one as “Very Good” (Table 1).
All hospitals had a voltage supply of 220V for single-phase and 380V for three-phase connections at 50Hz. Perceptions of voltage compatibility with MDs differed: two respondents rated it “Very Poor,” five “Poor,” seven “Acceptable,” four “Good,” and one “Very Good” and one did not know how the hospital voltage is compatible with MDs.
Table 1 Shows summary of the electrical access and safety3.3 Human resourceAccording to the respondents, the quantity of physicians in the surveyed facilities shows variation. The majority of respondents (58%) reported that one medical doctor is responsible for attending to more than 30 patients daily, followed by 16% who indicated that one doctor manages 20–30 patients per day. Across all facilities the ratio between medical doctors and patients was evaluated as “Very Poor” by 47% of respondents and “Poor” by 37% of respondents. This suggests a concerning shortage of medical doctors in meeting patient needs.
Moreover, the assessment revealed a deficiency of clinical officers and laboratory technicians in all the facilities assessed. These professionals are tasked with attending to more than 30 patients each day. The ratio of clinical officers and laboratory technicians to patients was rated as “Very Poor” and “Poor,” indicating an inadequate staffing level to address patient care needs.
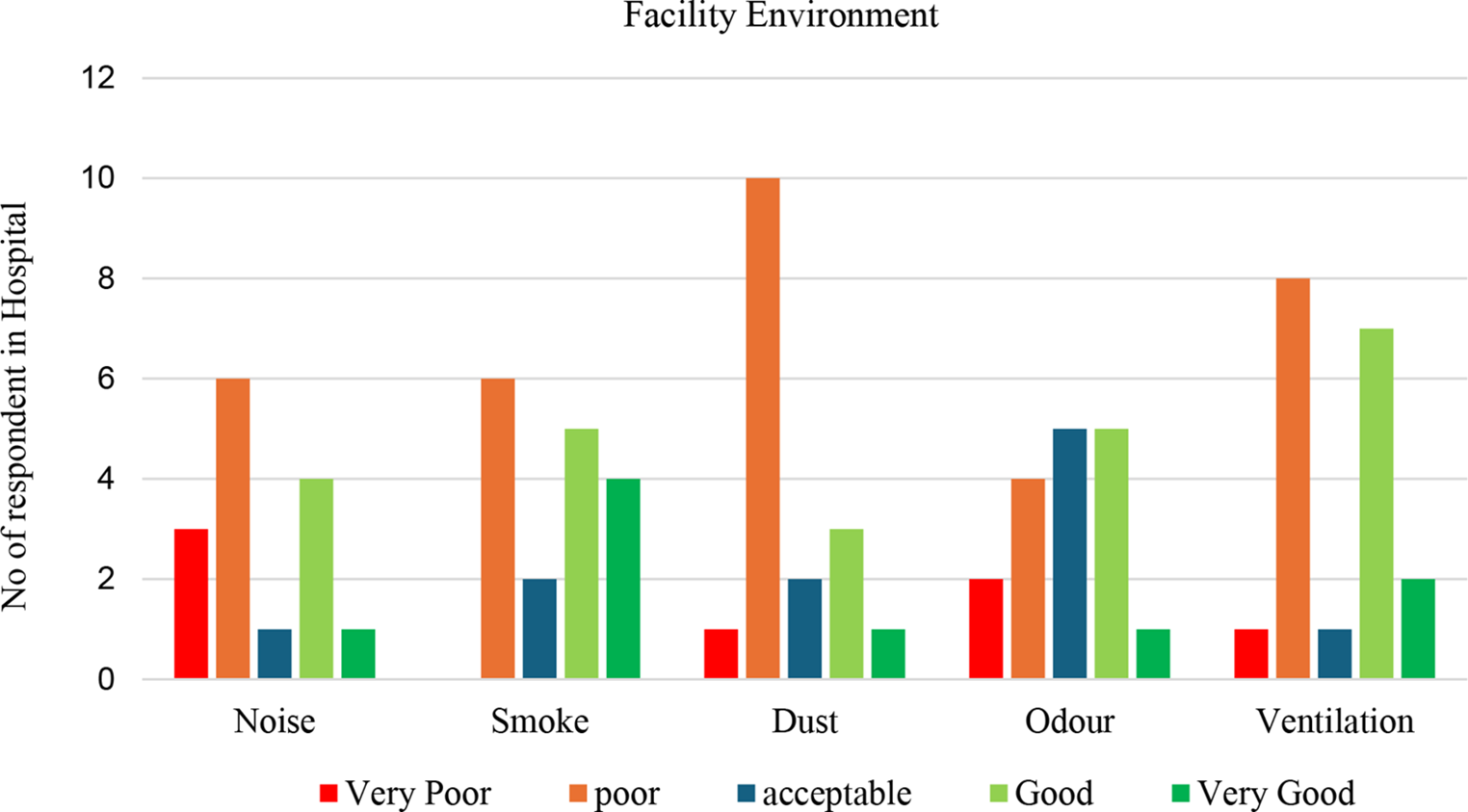
3.4 Facility environmentMost responses (Fig. 1) indicated a negative perception regarding the insulation or distance from facility excessive noise, smoke, dust, and unpleasant odours. Additionally, the adequacy of ventilation was largely deemed poor or very poor by a significant proportion of respondents.
Fig. 1
Graph below shows summary of Premises distance from Noise, Smoke, Dust, odour and ventilation
3.5 Waste disposalBased on the information provided by the respondents (Fig. 2), it appears that the frequency of cleaning in these facilities generally ranges from less than once a week or 1–2 times a week. However, five respondents mentioned that the facilities are undergo cleaning five or more times a week, indicating a higher frequency of cleaning in their respective environments.
Another issue raised relates to the materials utilized in the building. Respondents expressed varying perceptions of material quality concerning walls, ceilings, floors, and furniture. Among those who provided information on material quality, two rated it as “Very poor”, six as “Poor”, five as “Acceptable”, and five as “Good”. It is important to highlight that some respondents expressed uncertainty or lack of knowledge regarding the materials used within the building.
Fig. 2 3.6 Medical and electrical equipment
3.6 Medical and electrical equipmentIn 60% of the evaluated hospitals there were well-established biomedical engineering departments, however, the remaining 40% lacked such departments.
The number and variety of MDs differed across facilities, with each having a very different range of different devices available. For instance, Facility H11 and H18 (Both are primary hospital) do not have an x-ray machine, However, several other facilities (H2, H3, H8-H10, and H19) possess more than two x-ray machines, indicating a higher availability of this type of device in those hospitals. Colonoscopy and Gastroscopy equipment are absent in all facilities except for H4 and H10, each having one device. This discrepancy does suggest a varied availability of specialised equipment across the hospitals.
The overall observation highlights a lack of essential capital MDs, particularly in radiology and specific imaging areas. Devices mentioned include X-ray, CT scan, Colonoscopy, Gastroscopy, Ultrasound, ECG, and mammography. These devices play crucial roles in various medical procedures, diagnostics, but their availability seems limited in the facilities under assessment.
Additionally, there is a notable lack of regular maintenance scheduling across most facilities. For most medical equipment, inspections and preventive maintenance activities are performed less than once a year or only once a year. This infrequent maintenance schedule can increase the risk of equipment failures, reduce the overall reliability of devices, and could potentially compromise patient care.
Based on our survey data, 12 (65%) of the assessed facilities implemented a maintenance program for their medical equipment. This indicates that the majority of the facilities have established protocols for the upkeep and repair of their medical devices. However, it is concerning that the remaining eight (35%) do not have a maintenance program, suggesting a lack of a structured processes for equipment maintenance. Furthermore, despite the presence of maintenance programs, numerous MDs across all assessed hospitals are awaiting corrective maintenance (See Supplementary Material 1). This delay is primarily due to the shortage of spare parts and consumables, which are essential for replacing faulty parts or components in the equipment. The scarcity of consumables and spare parts hampers the timely repair and maintenance of medical devices, potentially leading to a prolonged downtime for medical equipment and affecting the quality of healthcare services provided.
3.7 Medical oxygen device systemThe primary sources of oxygen available in these facilities can be categorised as follows: in 70% of the facilities, oxygen is sourced from oxygen cylinders filled with compressed O2 gas. However, these cylinders would need to be refilled or replaced when its oxygen supply is depleted. In 20% of the facilities, they utilised oxygen concentrator machines, and in 10% of the facilities, there is an oxygen plant that serves as a central supply of oxygen for the patients.
The delivery of oxygen supply to healthcare facilities faces several various challenges. One significant issue arises from the predominant use of oxygen cylinders as the main source of oxygen in most facilities. Obtaining these cylinders from external sources can involve supply and logistical complexities which hinders their procurement. Transportation challenges, such as delays or disruptions in the delivery process, coupled along with budget constraints, can affect the consistent and timely provision of oxygen to healthcare facilities. This is supported by the respondents that indicated approximately 80% of the facilities face difficulties in maintaining a continuous oxygen supply due to supply chain and logistical problems. Fourteen hospitals further lack oxygen analysers, which are important devices for measuring and verifying oxygen concentration delivered to patients. Without an oxygen analyser, healthcare providers are unable to confirm the concentration of oxygen being delivered to patients. This lack of quality control increases the risk of the improper administration of oxygen, which can be harmful or ineffective in-patient care.
Another challenge arises from the limited accessibility to spare parts and consumables for the oxygen concentrators utilised in some of the assessed facilities. Table 2 illustrates the oxygen concentrator output and purity measured from six specific models of oxygen concentrators in NCSH during the survey, focusing on the YUWELL 7 F-5 (0.5–5 L/Min) model. The data collected by one of the authors revealed that the quality of the devices output was quite low and as a result it is damped in the workshop. Despite attempts to troubleshoot the device, it remained inoperable due to limited access to spare parts. “Oxygen concentrators require regular maintenance to ensure their continuous functionality and proper output of oxygen during patient care” said one of the senior biomedical engineers. Spare parts such as molecular sieve beds, inlet filters, flow meters, and valve blockages are crucial for repairing and maintaining oxygen concentrators. From the field note and answer to the survey as indicated in Fig. 3, the molecular sieve bed represents a significant challenge for 70% of the respondents, while 15% face difficulties with the inlet filter. The lack of access to these necessary spare parts and consumables can hinder the proper functioning of oxygen concentrators, impacting patient care.
Fig. 3
Component failure of oxygen concentrators according to respondents
Additionally, there is a requirement for capacity building and training in the maintenance and operation of oxygen supply devices. The respondent stressed that “proper training ensures that healthcare staff are equipped with the necessary skills to effectively maintain and troubleshoot the devices. However, the lack of training and capacity building programs for healthcare professionals can further contribute to challenges in maintaining the oxygen supply infrastructure and addressing issues that may arise.”
Several oxygen concentrator machines were left at the Nekemte Comprehensive Specialized Workshop, awaiting maintenance as indicated in Table 2, due to a shortage of various spare parts at the time of the visit.
Table 2 Oxygen concentrator oxygen purity output (these devices are stored in the workshop being going under maintenance during the visit)3.8 Data base handlingApproximately 65% of the assessed health facilities use paper-based systems for managing medical equipment, while 35% have adopted computer-based systems. Despite this, most respondents rated data management as “Poor” (39%) or “Very Poor” (26%), highlighting major deficiencies. Although some facilities record basic data like manufacturing year, acquisition date, and serial numbers, crucial information such as warranty duration, service dates, technical manuals, and European Conformity (CE) compliance is often missing.
留言 (0)