
記住我





Aim of the present study was to evaluate the influence of a manufacturer change in reverse fracture arthroplasty on patients` outcome as well as in the user collective of shoulder surgeons.
Despite including patients 65 years and older, a mean age of nearly 80 years was observed in both groups. This represents the current demographic trend of an aging society and suggests an age- and gender related affection of the outcome. Stenquist et al. found no difference in complications or functional outcomes between a younger (mean age 64 years) and older (mean age 78 years) collective of patients after reverse fracture arthroplasty, which underlines comparability [7].
The total length of inhospital-stay in both groups was not significantly different (9 vs. 10 days). These findings differ from results by Menendez et al., who stated a mean length of stay from 4 days after surgery for proximal humerus fracture (internal fixation or arthroplasty), but are consistent to studies from the authors country, where 11.5 and 14.6 days were noted after reverse fracture arthroplasty [8], [9]. Patient (age, comorbidities) and system (availability of surgical capacity, lack of postoperative ambulatory care) related factors may delay surgery and timing of discharge, so these differences could be attributed to variances in treated patients and treating countries.
No significant difference, but a clear trend in duration of surgery with decreased time (mean 104 vs 80 min) after change of manufacturer was observed. Other data on reverse fracture arthroplasty show a mean duration from 130 to 140 min. Our findings might be mainly attributed to cementless fixation of the stem after manufacturer change. Only in 4 cases of group B, there was a cemented fixation of the stem, which was caused by an insufficient metaphyseal anchorage or fracture in the calcar region. A reduced duration of surgery is already known with reduced occurrence of postoperative complications from other surgical procedures in the elderly and could be regarded as an unintentional benefit of manufacturer change [10], [11].
Various parameters were implemented in reverse shoulder arthroplasty to objectively compare baseline situation and postoperative results. One of them, the so called reverse shoulder arthroplasty angle (RSA), evaluates on preoperative radiographs the inclination of the inferior glenoid cavity. On postoperative radiographs, the filling of this gap is measured, which stands for correct baseplate inclination. An adequate correction of glenoid inclination is vital in correct implant positioning, as superior inclination is a risk factor for reduced range of motion, loosening, and instability [12]. Also functional outcome is influenced by the RSA, as patients with a postoperative RSA of 0–10° tended to better functional results [13]. To achieve neutral inclination of the baseplate, the preoperative RSA needs to be corrected.
With a mean preoperative RSA of 23° ± 6° in both groups (22.8° ± 6.4° vs. 23° ± 6.2°), our results are comparable to Boileau et al., who found a mean RSA of 25° ± 8 [14]. Postoperative RSA is also comparable to current literature in both groups with a mean of 11° ± 5° (10.5° ± 5.1° vs. 11° ± 5.7°). Uçan et al. found a mean RSA of 5.5 ± 10.1° in plain x-rays and of 10.4 ± 10.3° in CT-scans after surgery [13].
During follow-up, functional outcome showed no clinically relevant difference between the groups, both short and mid-term. Tuphe et al. report comparable results in an even longer follow-up period depending on the implementation of an early rehabilitation protocol [15].
Regarding overall complications as mentioned before, we observed no difference with changing manufacturers and found a comparable spectrum as stated in current literature [16].
Nevertheless, a detailed review of each specific complication is essential:
According to a review by Contreras et al. the incidence of periprosthetic infection after reverse shoulder arthroplasty ranges from 3 to 4%, although rates as low as 0.5% and as high as 6.7% have been reported [17]. Our study showed rates from 1% (Arthrex) to 2% (Tornier) and consequently a low overall periprosthetic infection rate regardless of the manufacturer.
The different application options of the stems are certainly the biggest difference between the two implants. Therefore, a close look at potential effects is necessary. In the present collective cementation changed from a necessity to a rescue option. At the same time, however, non-cementation may also harbor risks. Despite a case of stem loosening, the option of non-cementation is a big step forward, starting with the operation time and ending with better revisability. Our findings match with a systematic review by Phadnis et al. and their conclusion, that uncemented stems have at least equivalent clinical and radiographic outcomes compared with cemented stems when used for reverse total shoulder arthroplasty. They also report intra-operative humeral fractures (cemented: 0.5%, uncemented 1.2%) and stem loosening in several studies, so regardless of the implant, its fixation and surgical experience, this seems to occur in low quantity. With an intra-operative humeral fracture rate of 3% after change of manufacturer, also a learning curve should be considered in our collective. During implantation of the stem and inlay, supporting and neutralizing the elbow joint could reduce intra-operative fracture risk [18]. The authors also strongly recommend dosed impaction of the cementless stem and dosed insertion of the inlay. In addition, an intraoperative X-ray check for an iatrogenic fracture of the calcar is recommended. In doubt, cementation should be generously indicated.
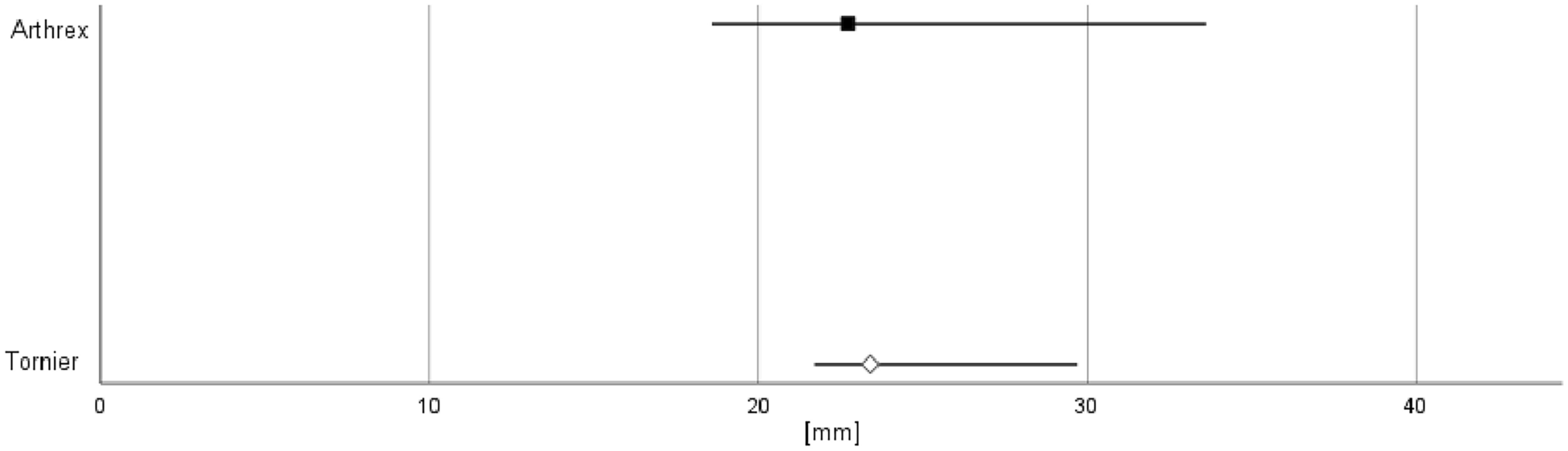
Scapular notching, once a mainly radiologic finding, gained clinically relevant importance with growing long-term data. The reported incidence varies widely, ranging from 4.6% to 96%, with decreasing rates in recent studies. It is more common in the 135° than in the 155° stems [19]. Our data showed a trend to less notching in 135° prosthesis, but without significant difference between the groups. Correct implantation technique (lateral offset with inferior overhang of the glenosphere) therefore is crucial in avoiding scapular notching, despite profound knowledge of the specific implant and manufacturer. As there are various options for lateralization (lateralize on the humeral, on the glenoid or on both sides), some authors aimed for a better definition and measured the global lateral offset, summing up both factors. They found high implant-depending variability among different manufacturers [20]. This is also proven by our data, that show significant difference in global lateral offset between the groups.
Another parameter, that primarily was noticed on radiographic follow-up and became outcome relevant with increasing data, is the tuberosity union rate. Patients with healed tuberosities after RSA in proximal humerus fractures showed improved range of motion and satisfaction [21]. After manufacturer change, a growing trend to tuberosity union was observed with 62% in the Tornier and 70% in the Arthrex group. In detail, we found higher tuberosity dislocation (27% Tornier, 20% Arthrex) than resorption (11% Tornier, 10% Arthrex) without significance.
Apart from all radiographic parameters, human factors are crucial for correct use of each implant and have a big impact on the outcome. Considering the team working together in the operation room, the scrub nurse as well as the surgeon have to know specific features of a new implant and how to use them. Nyberg et al. evaluated the experiences of operating room nurses and they stated to help solve problems as they arise, where there are obvious risks for patient complications [22] (Fig. 4).
Fig. 4
Applicability by the OR nurse [Grade 1–6]
留言 (0)