
記住我





In the following, the results are described separately according to the analyses carried out.
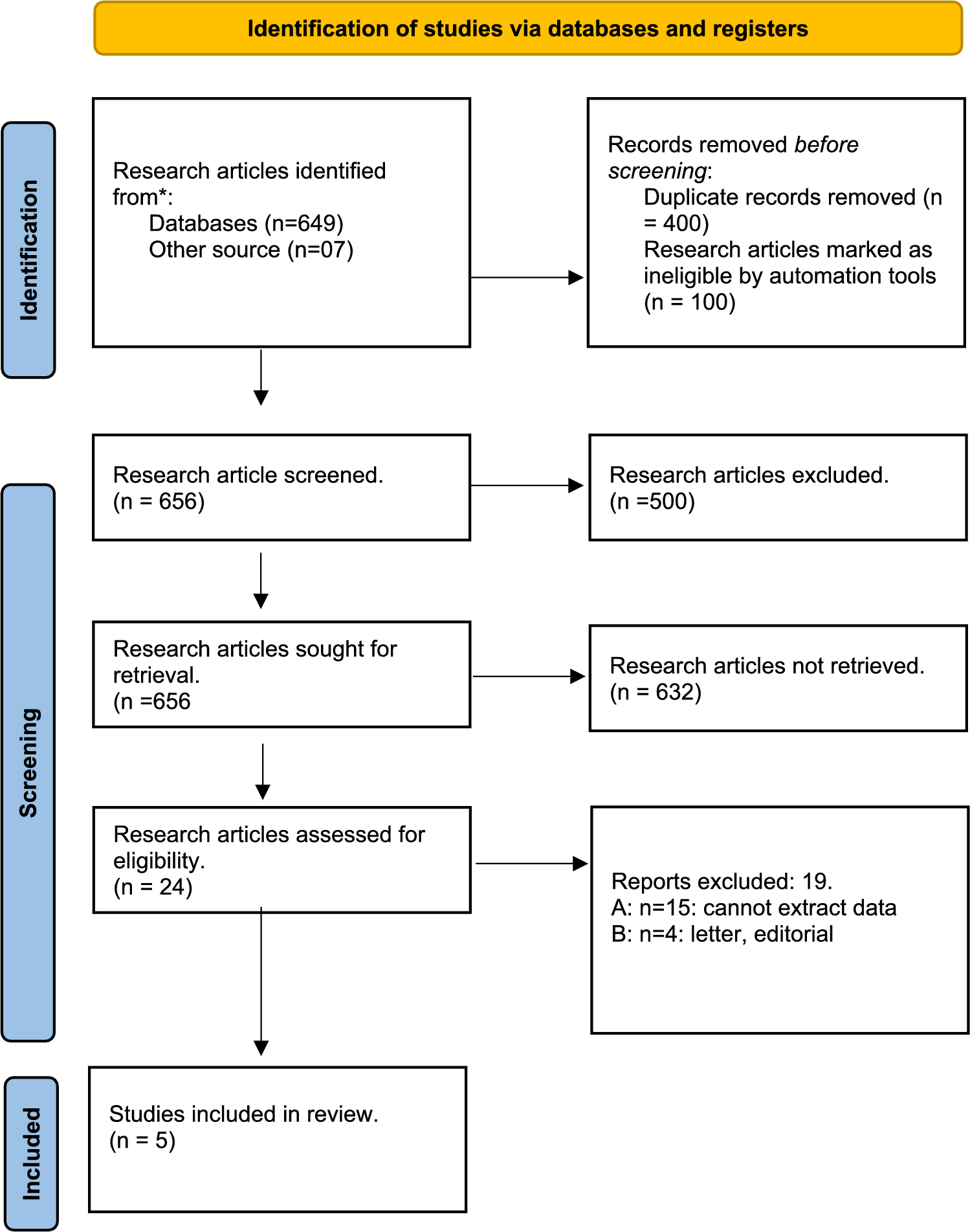
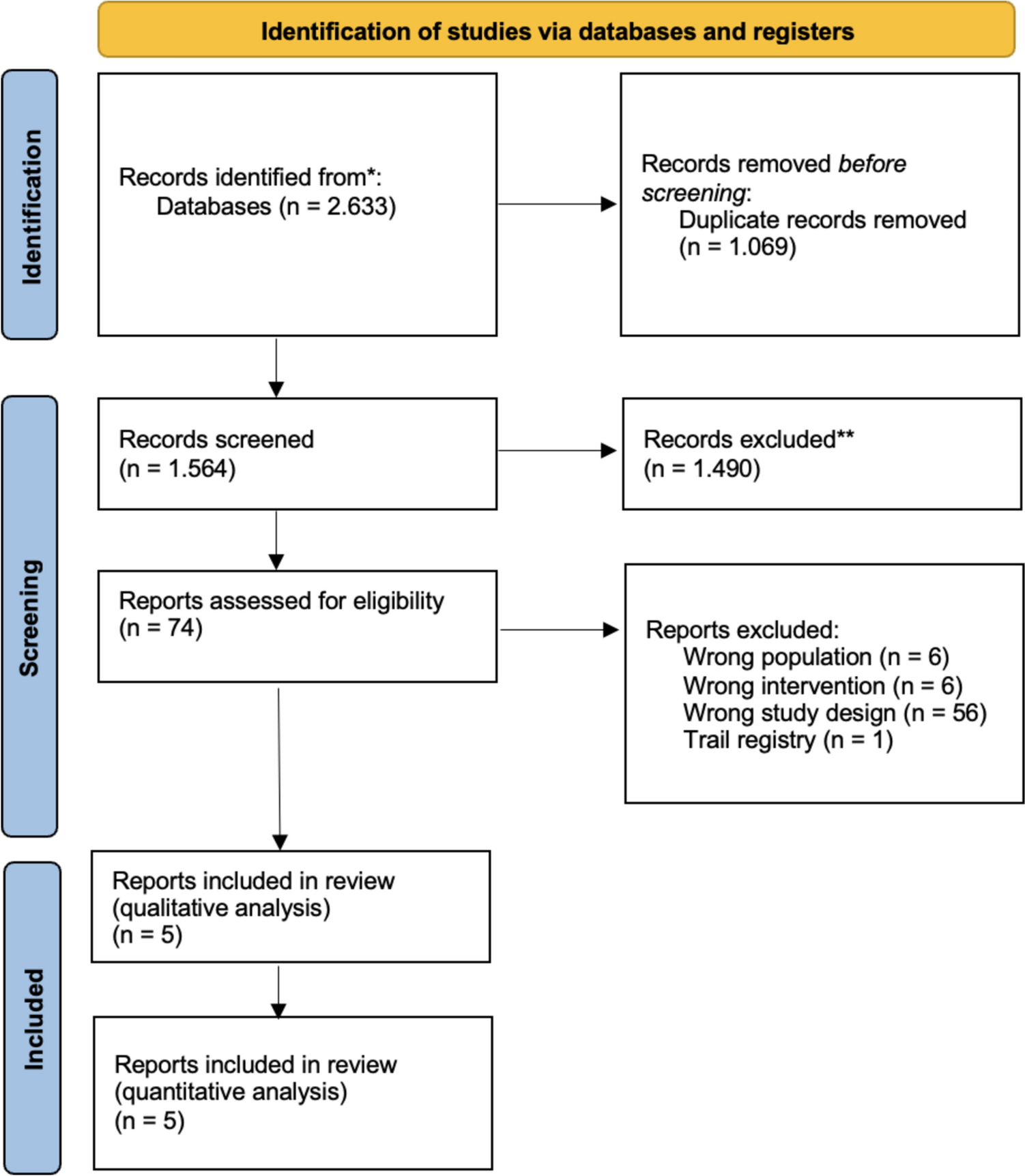
Study selectionThe search returned 1,564 results whose titles and abstracts were screened. A full text screening was then carried out on 74 of these studies, of which 69 were excluded as they did not meet the inclusion criteria. Reasons for exclusion were wrong study population (n = 6), wrong intervention (n = 6), wrong study design (n = 56) and trial registry (n = 1). Five studies were included in the qualitative review and the quantitative analysis. Figure 1 illustrates the entire review process.
Fig. 1
Flowchart of the systematic review selection process
Study characteristicsThe five RCTs [4, 6, 13,14,15] had a total of 335 adult participants, with a majority being male (82.7%). All patients were diagnosed with severe multiple-trauma and had a femur fracture (despite 5 patients with tibial fracture [14]) that required treatment. The age of patients in the various studies demonstrated some variation and the average age ranged from 28 years to 41.6 years. A summary of the study characteristics can be found in Table 1.
Table 1 Study characteristics of the included studies [4, 6, 13,14,15]During the analysis, it became evident that the concept of early versus late stabilization encompassed two distinct concepts. The first comprises the immediate surgical stabilization versus delayed surgical stabilization, the second primary intramedullary nailing (IMN; ETC concept) versus primary external fixation (EF) with delayed IMN (DCO concept). The relevant studies were segregated into distinct groups and subjected to separate analyses.
Immediate stabilization versus delayed stabilization of femoral fracturesRisk of bias in studiesThere were some concerns regarding the overall risk of bias among the included RCTs [6, 14]. The reason for this in all studies was the evaluation of some concerns related to the randomization process and the selection of reported results. However, a high risk was not found in any of the studies.
Summary of findingsImmediate stabilization compared to delayed stabilization in adult polytrauma patients (Table 2).
Table 2 Summary of findings immediate stabilization versus delayed stabilizationOverall mortalityTwo studies reported on the overall mortality for 100 participants [6, 14] (Fig. 2). Following the results out of the included RCTs, it remains uncertain whether immediate stabilization compared to delayed stabilization increases or decreases overall mortality (RR 1.37, 95% CI 0.24–7.87; risk difference (RD) 60 per 1.000, 95% CI 10 fewer to 342 more; 2 studies, I2 = 0%, very low certainty of evidence). Reasons for downgrading were very serious risk of bias and serious imprecision.
Fig. 2
Forest plot describing the difference between early stabilization compared to late stabilization regarding overall mortality in the included studies [6, 14]. CI = confidence interval
Clinical status: improvement of admission rate on ICUOne study reported on the improvement on the admission on the ICU for 83 participants [6] (Fig. 3). Due to downgrading, including the results out of this RCT, it remains uncertain whether immediate stabilization compared to delayed stabilization increases or decreases the rate of admission on the ICU (RR 0.56, 95% CI 0.42–1.03; RD 392 per 1.000, 95% CI 250 fewer to 612 more, 1 study, heterogeneity not applicable). Our main reason for downgrading was very serious risk of bias and very serious imprecision.
Fig. 3
Forest plot describing the difference between early stabilization compared to late stabilization regarding improvement admission on ICU in the included study [6], CI = confidence interval
ICU length of stayThe results from the included studies [6, 14] do not support statistical analysis for this outcome. However, the results from Bone et al. enable a narrative comparison: Patients who received early stabilization of multiple injuries (n = 46) had a shorter ICU stay, averaging 2.8 days, compared to those who received late stabilization (n = 37), who spent an average of 7.8 days in the ICU.
Hospital length of stayThe results from the included studies [6, 14] do not support statistical analysis for this outcome. However, the results from Bone et al. enable a narrative comparison: The total hospital stay was shorter for the early stabilization group, with an average of 17.3 days, in contrast to 26.6 days for the late stabilization group.
ETC versus DCO on femoral fracturesRisk of bias assessmentThere were some concerns regarding the overall risk of bias among the three RCTs [4, 13, 15]. Reason for this was the evaluation of some concerns in both studies regarding measurement of outcomes. In one study, the randomization process and the selection of the reported results were also assessed with some concerns [13], in the other the deviation from the intended intervention [4, 15].
Summary of findingsSee Table 3.
Table 3 Summary of findings femoral nailing versus external fixationClinical status: duration to liberation from IMVTwo studies reported on the liberation from IMV for 199 participants [13, 15] (Fig. 4). We found that primary femoral nailing (ETC) compared to external fixation (DCO) may decrease duration to liberation from invasive mechanical ventilation, compared to external fixation (RR − 3.94, 95% CI − 6.39 to − 1.49; RD 3.94 days lower, 95% C 6.39 fewer to 1.49 more, 2 studies, 199 participants; I2 = 0%; low certainty of evidence). Our main reason for downgrading were serious risk of bias and serious imprecision.
Fig. 4
Forest plot describing the difference between femoral nailing (ETC) compared to external fixation (DCO) regarding the improvement on improvement on duration to liberation from IMV in the included studies [13, 15]
ICU length of stayThree studies reported on the improvement regarding the ICU length of stay for 199 participants [4, 13, 15] (Fig. 5). We found that primary femoral nailing (ETC) compared to external fixation (DCO) may decrease the ICU length of stay compared to external fixation (RR − 5.40, 95% CI − 9.84 to − 0.95; RD 5.4 days lower, 95% C 9.84 fewer to 0.95 more, 3 studies, 199 participants; I2 = 27%; low certainty of evidence). Our main reason for downgrading were serious risk of bias and serious imprecision.
Fig. 5
Forest plot describing the difference between primary femoral nailing (ETC) compared to external fixation (DCO) regarding the improvement on ICU length of stay in the included studies [4, 13, 15]
Hospital length of stayOne study reported on the hospital length of stay for 33 participants [15] (Fig. 6). Regarding the results out of this RCT it remains uncertain whether primary femoral nailing (ETC) compared to external fixation (DCO) increases or decreases hospital length of stay (RR − 2.10, 95% CI − 15.20 to 11.00; RD 2.1 days lower, 95% CI 15.2 fewer to 11 more, 1 study, 33 participants; heterogeneity: not applicable). Our main reason for downgrading were serious risk of bias and extremely serious imprecission.
Fig. 6
Forest plot describing the difference between femoral nailing (ETC) compared to external fixation (DCO) regarding the improvement on improvement on hospital length of stay in the included study [15]
留言 (0)