Participants
Participants with DBDs and unaffected controls aged 8–18 years were recruited across four sites [Nijmegen (Radboud University Medical Center and the Donders institute for Brain, Cognition and Behavior, Nijmegen, The Netherlands), Mannheim (Central Institute of Mental Health, Mannheim, Germany), London (Centre for Neuroimaging Sciences, Institute of Psychiatry, Psychology and Neuroscience, King’s College London, London, United Kingdom; Department of Child Psychiatry, Institute of Psychiatry, Psychology and Neuroscience, King’s College London, London, United Kingdom), and Barcelona (Department of Child and Adolescent Psychiatry and Psychology, Neurosciences Institute, Hospital Clinic de Barcelona, Barcelona, Spain)], as part of the EU FP7 MATRICS and Aggressotype projects (http://www.matrics-project.eu; http://www.aggressotype.eu/). Detailed information about recruiting sites and subjects included in the analysis can be found in supplementary data (Table SI1).
Participants were included as DBD cases if they met criteria for an ODD and/or CD diagnosis on the Kiddie Schedule for Affective Disorders and Schizophrenia Present and Lifetime Version (K-SADS-PL) [38], based on the Diagnostic and Statistical Manual of Mental Disorders (fifth edition, DSM-5) criteria, or scored higher than a clinical cut-off (T ≥ 70) on the aggression or rule-breaking subscale of the Teacher Report Form (TRF), Youth Self Report (YSR), or Child Behavior Checklist (CBCL) [39]. Inclusion criteria for unaffected controls were the absence of a DSM-5 Axis-I disorder based on the K-SADS-PL [38], and aggression scores T < 70 on the aggression or rule-breaking subscales of the TRF, YSR, and CBCL [39]. IQ of the participants was estimated by using four subtests (vocabulary, similarities, block design, and picture completion/matrix reasoning) of the Wechsler Intelligence Scale for Children III or IV [40, 41].
Exclusion criteria for both unaffected controls and DBD cases included contraindications for MRI, an IQ < 70 [40, 41], and/or a primary DSM-5 diagnosis of psychosis, bipolar disorder, major depression, or anxiety disorder. After the description of the study, written informed consent was obtained from parents, and from participants who were older than 12 years old, in accordance with local legislation. The study has been approved by the local ethics committee at each site. Information about medication use was collected during the interview with the parents on the testing day.
Rating scales
The CBCL is a widely used 113-item parent-completed questionnaire evaluating behavioral competency and behavioral problems in children within the past six months [39]. Responses are rated on a three-point Likert scale. In this study, DBD symptom severity score was calculated as the sum of all eight items for conduct problems and all five items for oppositional defiant problems. The Swanson, Nolan, and Pelham Rating Scale (SNAP-IV) is a 26-item parent-rated measure used to assess ADHD and ODD symptoms in children [42]. It includes nine items for the symptoms of ADHD hyperactive-impulsive type and nine items for the symptoms of ADHD inattentive type as specified in DSM-V. The items are scored on a four-point Likert scale. ADHD symptom severity score was calculated as the sum of average rating-per-item subscale scores for the inattention and hyperactivity-impulsivity.
To examine possible confounding effects of aggressive behaviors as well as callousness, uncaringness, and unemotionality, the self-reported the Reactive-Proactive Aggression Questionnaire (RPQ) [43], and the Inventory of Callous-Unemotional Traits (ICU) [44] were used to measure reactive and proactive aggression, and callous-unemotional traits, respectively.
fMRI paradigm: stop-signal task
The stop-signal task has been used for many years to probe the behavioral and neural mechanisms of response inhibition [9]. Using the visual version of this paradigm, participants performed a two-choice reaction task in which they were required to inhibit their ongoing response when they were presented an additional stimulus, a stop-signal, following a target stimulus, a go-signal. In trials with a go-signal (go trials), a horizontal left- or right-pointing arrow was displayed for a maximum of 2500 ms or until a button was pressed. Depending on the direction of the arrow, participants were asked to respond as quickly as possible by pressing the left or right button using their right index finger. In 20–25% of trials (stop trials), an arrow pointing upwards was presented after a variable delay after the appearance of the go-signal, the so-called “stop-signal delay”, indicating that participants were required to interrupt the already initiated reaction and to suppress their responses. We used a performance-adjusted stop-signal task in which the initial 250-ms stop-signal delay was continuously adapted to the individual response time of the participant by increasing or decreasing it 50 ms after a successful or unsuccessful stop trial, respectively, so that an approximately 50% success rate on the stop trials for all participants was achieved [45]. Before scanning, subjects were asked to complete a short practice session of the stop-signal task. The experimental task consisted of 156 go- and 40 stop-trials and the duration of the experiment was approximately 12 min, with a range of 10 to 13 min.
Response inhibition performance was measured by the stop-signal reaction time (SSRT), which was calculated by subtracting the mean stop-signal delay from mean reaction time [45]. Other task outcomes of interest were mean reaction time to go-stimuli (MRT), intra-individual coefficient of variation of reaction time to go stimuli (ICV), the percentage of omission errors in the go trials (Go error), and the percentage of commission errors in the stop trials (Stop error).
MRI acquisition and processing
MRI scans were performed using 3-Tesla MR scanners across imaging sites with the scanning parameters reported in supplementary Table SI2 and Table SI3. The fMRI data were preprocessed using FSL FEAT (FMRIB’s Software Library, www.fmrib.ox.ac.uk/fsl; fMRI Expert Analysis Tool, version 6.0) [46]. Preprocessing included removal of the first five volumes of each acquisition, motion correction to the middle volume, slice-timing correction, and spatial smoothing using a 6-mm Gaussian kernel. After preprocessing, additional motion artifacts were removed by applying the ICA-AROMA protocol, which is freely available through GitHub (https://github.com/maartenmennes/ICA-AROMA) [47].
Behavioral data analysis
Multiple linear regression analyses were conducted to examine the relationship between behavioral outcomes of the stop-signal task ((i) mean reaction time to go-stimuli, (ii) intra-individual coefficient of variation of reaction time to go stimuli, (iii) percentage of omission errors, iv) stop-signal reaction time, v) percentage of stop errors) with the DBD and ADHD symptom severity scores while controlling for sex, age, IQ, scanning site, and the other respective score dimension, using the lme4 package in R (version 4.0.2) [48, 49]. In total, 10 analyses (5 stop-signal task behavioral outcomes in relation to 2 symptom scores) were performed.
fMRI data analysis
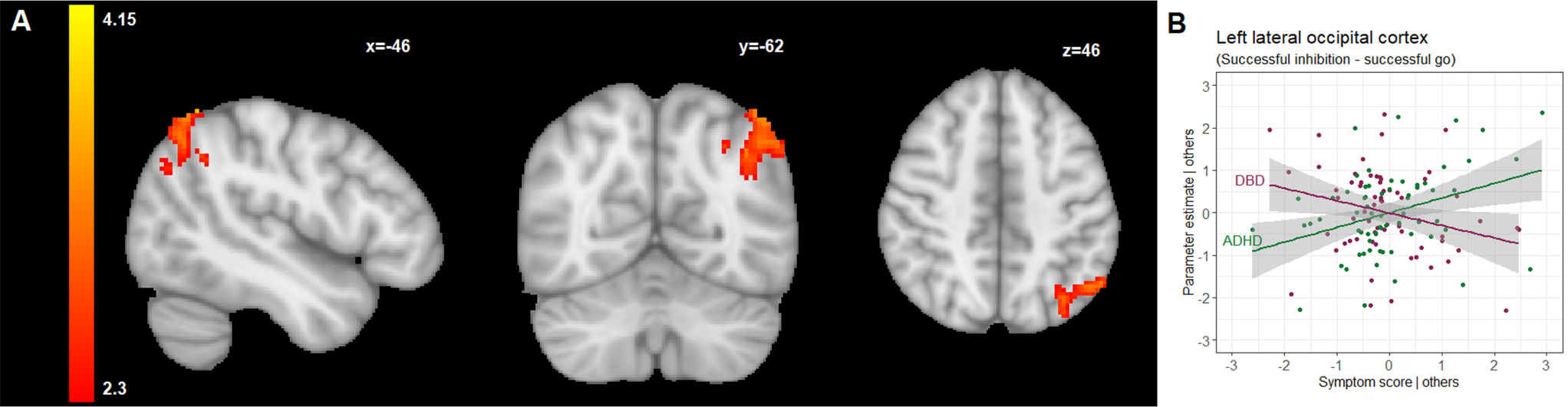
The individual-level analysis was conducted across all participants using a general linear model in FSL FEAT [46]. The model included three regressors of interest (onsets of go-signals in correct go-trials successful and unsuccessful stop trials, separately) and two regressors of no interest (onsets of go-signals in incorrect and miss go trials together, and white matter and cerebrospinal fluid time series as nuisance regressors). The motion parameters were not included as regressors of no interest as we excluded participants with excessive head motion (> 3 mm) and applied ICA-AROMA for the automatic detection and removal of motion-related artifacts from the fMRI data [47]. Each regressor was convolved with a canonical hemodynamic response function, and the temporal derivatives of the regressors were also added as regressors in the model. Activation maps of three complementary contrasts of interest were calculated and spatially normalized to the MNI template to be used in group-level analysis. The three contrasts were: successful inhibition versus successful go (successful stop-trials versus successful go-trials to isolate the activation of successful inhibition of motor responses versus processing of a stimulus (the go-trial serves as reference), to identify brain regions that are activated in successful response inhibition), failed inhibition versus successful go (unsuccessful stop-trials versus successful go-trials to isolate activation of failed inhibition of motor responses versus processing of a stimulus (again, the go-trial serves as reference), to identify brain regions that are activated when the participant fails to inhibit a prepotent response), and successful inhibition versus failed inhibition (successful stop-trials versus unsuccessful stop-trials to isolate activation differences between successful and failed inhibition of motor responses, to identify brain regions where activation is different in successful and failed response inhibition).
In the group-level analysis, mixed-effects analysis using FLAME 1 (FSL’s Local Analysis of Mixed Effects) [50] were conducted to generate t-contrasts with the contrasts mentioned above to determine the influence of DBD and ADHD symptom severity on response inhibition-related brain activation during the stop-signal task. For this, we used either the DBD or the ADHD symptom severity scores as regressor of interest, while controlling for sex, age, IQ, scanning site and the other (DBD or ADHD) symptom dimension. A total of 6 analyses were performed (3 fMRI contrasts for 2 predictors of interest). To investigate global, cluster-wise effects across the brain, a cluster-forming threshold was applied to Z-statistic images at the FSL default value of Z = 2.3. To correct for multiple comparisons across the whole brain, family-wise error (FWE) corrected P values were computed for each cluster and thresholded at P = 0.05. Then, for every participant, the mean parameter estimates for all clusters positively or negatively associated with DBD or ADHD symptom severity were extracted, and post-hoc analyses were carried out using R software to explore the associations further [48]. In the case of a cluster associated with ADHD symptom severity scores, the link between cluster means and DBD symptom severity scores was also explored, and vice versa. This was done to investigate, whether clusters of brain activity identified to be relevant for one disorder (even while controlling for the other disorders’ symptomatology), could be potentially also relevant for the other disorder. For these post-hoc analyses, False Discovery Rate (FDR) correction was applied (FDR P-value threshold 0.05) to the P-values of the regression beta coefficients for the symptom scores as predictor in relation to the brain cluster means as outcome.
Correlation of behavioral performance with brain activation
In order to establish a link between neural activity and behavioral performance, partial correlations between parameter estimates extracted from the clusters and behavioral measures ((i) mean reaction time to go-stimuli, (ii) intra-individual coefficient of variation of reaction time to go stimuli, (iii) percentage of omission errors, iv) stop-signal reaction time, v) percentage of stop errors) were calculated, partialling-out the effect of sex, age, IQ, scanning site, and DBD and ADHD symptom severity scores. A total of 45 correlations were computed (9 brain clusters with 5 behavioral measures).
Analyses of potential confounding factors and sensitivity analyses
To rule out a possible confounding effect of aggressive behavior and callous-unemotional traits among the participants, additional sensitivity analyses for the identified brain clusters were conducted by additionally correcting for total scores on the RPQ [43] or the ICU [44], in addition to sex, age, IQ, and scanning site, and DBD and ADHD symptom severity as the variables of interest (see Supplement I, available online). A total of 36 analyses (9 brain clusters with 2 symptom scores with additional correction for RPQ scores and 9 brain clusters with 2 symptom scores with additional correction for ICU scores) was performed here.
To exclude a potential effect of stimulant (methylphenidate and/or lisdexamphetamine) use, identified brain clusters were analyzed after excluding participants who used stimulant medication on the testing day (see Supplement I, available online). A total of 18 analyses (9 brain clusters with 2 symptom scores) was performed here.
To investigate whether the identified relations between task-related brain activation and DBD and/or ADHD symptom severity were driven by residual motion artefacts in the data, we computed the average FD-value for the participants included in the analyses and analyzed the correlation of the FD-values with ADHD and DBD symptom severity.
Furthermore, differences between in- and excluded participants on a number of key variables were investigated because of the relatively large number of exclusion due to data quality control.




留言 (0)