Participants
The current study used data from the Growing Up in Ireland (GUI) Infant Cohort ‘08, which is a nationally representative sample of 11,194 children born in Ireland between December 1, 2007, and June 30, 2008. The GUI project was administered by trained Officers of Statistics from the Irish Central Statistics Office, and recruitment and data collection were carried out using face-to-face household interviews in a manner akin to the approach used for the Census of the Population. Ethical approval for the project was overseen by the Irish Department of Children and Youth Affairs. Caregivers provided informed consent and received no financial incentive for study participation. Families were recruited when the child was 9 months old and followed up thereafter at two-year intervals. The constructs of interest for this study are from waves one to five (i.e., 9 months, 3, 5, 7, and 9 years). Detailed information on the sampling and scope of GUI is available at: https://www.growingup.gov.ie/.
At 9 months, 11,134 participants completed the survey. The final sample for this study included 10,170 participants who had at least one internalizing and externalizing symptom measure in childhood (waves 2–5) (91.3% of the original sample at 9 months). To assess whether loss to follow-up had been random or selective, those who dropped out (N = 964) were compared to those who were retained in the study (N = 10,170). Those lost to follow up and those who retained in the study were similar in terms of the percentages of female (N = 451, 46.8% vs. N = 5004, 49.2%, p = .151). However, those lost to follow up were more often from a non-Irish background (N = 397, 41.7% vs. N = 1883, 18.6%, p <.001), and had the lowest quintile of annual income (N = 297, 34.9% vs. N = 1922, 20.4%, p <.001) than those retained in the study.
Measures
Internalizing and externalizing symptoms across childhood. Internalizing and externalizing symptoms were measured using the Strengths and Difficulties Questionnaire (SDQ), which was completed by parents at four assessment points when children were 3, 5, 7 and 9 years. The SDQ is a widely used and psychometrically valid behavioral screening tool suitable for community samples [31]. In line with recommendations [32], internalizing symptoms were assessed by combining the 5-item negative emotionality (e.g., ‘child has many worries’) and the 5-item peer problems (e.g., ‘often fights with other children or bullies them’) sub-scales. Scores for each of the 10 items (0 = not true, 1 = somewhat true, 2 = certainly true) were added to derive a total score ranging from 0 to 20. Externalizing symptoms were assessed by combining the 5-item conduct problems (e.g., ‘child often cheats or lies’) and the 5-item hyperactivity (e.g., ‘child is easily distracted’) sub-scales, scored in the same way to derive a total score ranging from 0 to 20.
Regulatory problems at 9 months. Parents reported on their infants’ crying problems using the following question: ‘Do you feel that baby’s crying is a problem for you?’ The response scale (1 = yes; 2 = no) was recoded to reflect a crying problem (0 = no; 1 = yes). Parents reported on sleeping problems of their infants using the following questions: (a) ‘Is your baby ever difficult when put to bed?’ The original response scale (1 = most of the time; 5 = never) was recoded to a dichotomous response reflecting the presence of a sleeping problem (0 = never, often, at times, rarely; 1 = most of the time); (b) ‘How often does your baby wake at night?’ The response scale (1 = never; 5 = more than once per night) was recoded to reflect a sleeping problem (0 = never, occasionally, most nights, every night; 1 = more than once per night); (c) ‘How much is baby’s sleeping pattern or habits a problem for you?’ The response scale (1 = a large problem; 4 = no problem at all) was recoded to reflect a sleeping problem (0 = no problem at all, small problem, moderate problem; 1 = a large problem). The Cronbach alpha of these three items reflecting sleeping problems was 0.81. For sleeping problems, these three questions were summed, and dichotomised (0 = no sleep problems; 1 = 1, 2, or 3 sleep problems). Afterwards, crying and sleeping problems scores were summed to create a regulatory problems score: 0 = no regulatory problems, 1 = single regulatory problems (either crying or sleeping); 2 = multiple regulatory problems (co-occurrence of crying of sleeping).
Excessive screen media exposure at 3 years. Caregivers reported the time children spent watching television and using electronic devices when the children were 3 years of age with the following prompt: ‘Typically, how many hours a day does < child name > sit and watch television or videos/dvds?’. Screen exposure time was reported by caregivers in minutes and was categorized as follows: a) > 1 h per day (0: <= 60 min; 1: >60 min) based on WHO guidelines [21]; and b) > 2 h per day (0: <= 120 min; 1: >120 min) based on AAP guidelines [22].
Covariates. The following demographic variables were used as covariates: child sex at birth (0 = male, 1 = female), equivalized annual income quintiles (1 = lowest; 2 = 2nd; 3 = 3rd; 4 = 4th; 5 = highest), majority ethnicity: parent-reported ethnic status (0 = non-Irish including any other White background, African or any other Black background, Chinese or any other Asian background, Other including mixed background; 1 = Irish), marital status at 9 months (0 = single parenting; 1 = cohabiting, married), and second or later born (0 = first born, 1 = second or later born) entered as categorical variables, and gestational age (weeks) and age of the main carer at birth as continuous variables. Further, maternal psychological distress was assessed at 9 months using the Kessler Psychological Distress Scale [33], a widely used brief screening tool for mental health problems in the general population. It includes 6 items (e.g., ‘How often did you feel hopeless?’) rated on a 5-point scale ranging from ‘none’ to ‘all of the time’ that assess psychological distress in the past 30 days. A mean value was computed, with higher scores reflecting higher symptoms of mental health problems.
Statistical analysis
Descriptive statistics were used to summarize the characteristics of the sample. To estimate the differences between infants with and without any regulatory problems at 9 months of age in terms of outcome variables (i.e., internalizing and externalizing symptoms), covariates, and the potential moderator (i.e., screen media exposure), we performed independent samples t-tests for continuous variables and chi-square test for categorical variables using SPSS 27 (IBM Corp., Armonk, NY, USA). To address our main hypothesis, we followed a two stage process [8] as described in Jung and Wickrama (34). To address missing data, we used a maximum likelihood estimator and missing data were replaced using the full information maximum likelihood procedure.
Stage one
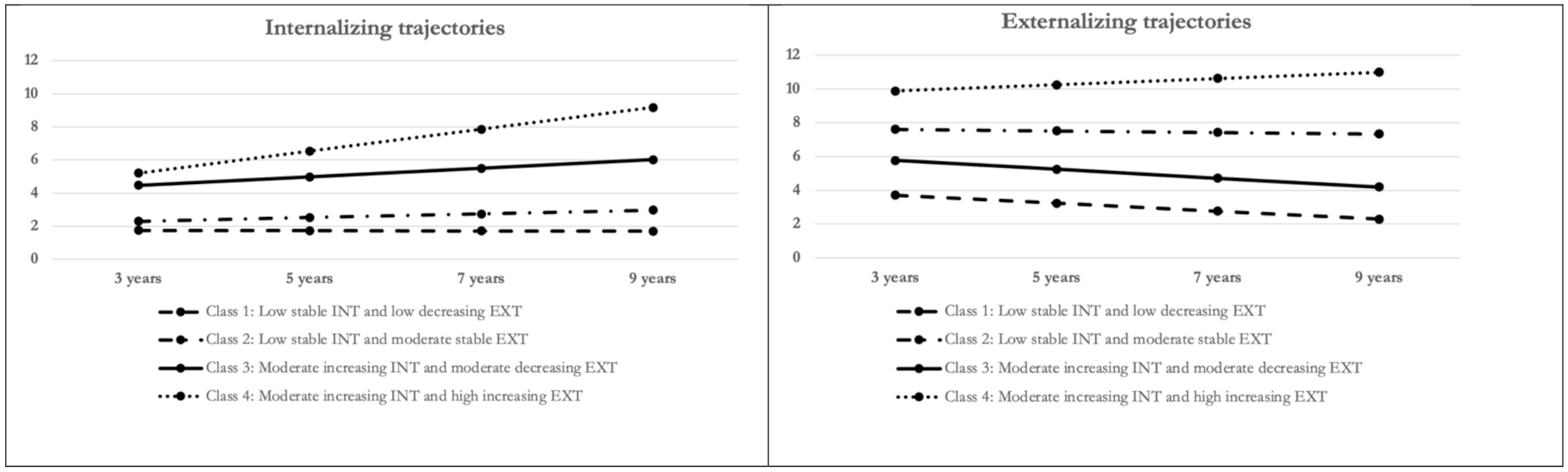
In stage one, we conducted parallel process latent class growth analysis (PP-LCGA) [30] to identify distinct groups of children exhibiting similar longitudinal patterns of co-developing internalizing and externalizing symptoms. This analysis was performed using MPlus (version 8, Muthen & Muthen, Los Angeles, CA, USA). PP-LCGA is a special case of growth mixture modeling that assumes homogeneity of growth parameters within each latent subgroup. Consequently, it can discern homogenous classes defined by different developmental trajectories of co-developing symptoms. The full information maximum likelihood approach was used to impute missing data.
The child’s sex at birth was incorporated as a covariate in the PP-LCGA due to previous evidence indicating sex differences in the development of internalizing and externalizing symptoms [29], which helped to avoid misspecification of subjects into latent classes [34]. We used the automatic R3STEP approach to model sex as an auxiliary variable, which adjusts for the impact of covariates while estimating the number of latent classes. This approach has been shown to produce less-biased estimates than traditional methods [35]. Other confounding variables were not included at this stage due to the considerable computational intensity required to estimate PP-LCGA models.
To determine the optimal number of latent classes, we examined several model fit indices, including Bayesian information criterion (BIC) and Akaike information criterion (AIC), Lo–Mendell–Rubin (LMR), Vuong–Lo–Mendell–Rubin (VLMR), and the entropy value [34]. Briefly, we estimated one to six classes and selected the best fitting model based on fit indicators. In addition to statistical model fit indices, several other criteria were considered to determine the optimal number of latent classes, including ensuring the smallest class should include at least 5% of the sample, the parsimony of models, their interpretability, and theoretical justification [17, 29].
Stage two
For stage two, we derived latent classes, saved them in a data file, and imported them into SPSS 27 for further analysis. We used the imported internalizing/externalizing classes to examine associations with predictors and internalizing/externalizing symptom classes across childhood. We conducted multinominal logistic regression analysis following the procedure outlined by Aiken and West [36]. This involved three steps: (a) including covariates (i.e., female sex, ethnicity, maternal psychological distress, income, gestational age, parity, marital status) and regulatory problems (i.e., single, multiple); (b) including excessive screen media exposure in early childhood (‘<=1 hour vs. > 1 hour’, and ‘<= 2 hours vs. > 2 hours’); and c) incorporating interaction terms between regulatory problems and the two levels of excessive screen media exposure.
Interpretation
We estimated the odds of membership in each latent class at different levels of our independent variable (infant regulatory problems) and moderating variable (excessive screen media exposure). Regarding regulatory problems, the OR represents the odds of class membership when an infant has any regulatory problems (i.e., either single or multiple regulatory problems) in comparison to not having regulatory problems. Regarding excessive screen media exposure, the OR represents the odds of class membership when a child was exposed to excessive screen media in comparison to no excessive screen media exposure. Given the likelihood of finding significant P values < 0.05 for small effects when using large sample sizes (N > 10,000), the results are interpreted both in terms of their magnitude (i.e., effect size) and respective 95% confidence intervals (CIs) [24].
Further analysis
To facilitate a clearer interpretation of the results, we additionally calculated the unadjusted and adjusted odds of class membership using children with ‘regulatory problems at 9 months and no excessive screen media exposure at 3 years’ as the reference group relative to ‘children with regulatory problems at 9 months and excessive screen media exposure at 3 years (separately for more than 1 or 2 hours of exposure)’.




留言 (0)