2.1 Study Design, Participants, and Interventions
ARC-HD was an open-label, single-arm, two-cohort, multicenter study. It was conducted from November 2013 to August 2017 at 37 sites in the USA, Canada, and Australia and consisted of two cohorts: the rollover cohort and the switch cohort. The study design and inclusion criteria for both studies have been described previously [14,15,16]. Briefly, the Rollover cohort comprised participants who had successfully completed First-HD [14], including participants randomly assigned to placebo and those randomly assigned to deutetrabenazine for 12 weeks. Key inclusion criteria for First-HD were age ≥ 18 years, HD diagnosis with at least moderate chorea (TMC score ≥ 8 and a total functional capacity [TFC] score ≥ 5), and no tetrabenazine use for ≥ 6 months prior to screening. Participants were required to have daily access to a caregiver, or a live-in caregiver in more advanced cases (TFC score 5–7). In ARC-HD, participants in the rollover cohort completed a 1-week washout period before initiating deutetrabenazine (6 mg/d), followed by re-titration for 8 weeks. Dosages could be titrated up or down in weekly increments of 6 mg/d up to 48 mg/d. After a dosage of 48 mg/d was reached, weekly changes of 6 or 12 mg/d [up or down, up to a maximum of 72 mg/d (36 mg twice daily)] were permitted at the investigator’s discretion to reach an optimal, individualized dosage on the basis of efficacy and tolerability. Dosages of 6 mg/d were administered once daily in the morning, and dosages ≥ 12 mg/d twice daily, approximately 10 h apart. If participants were receiving a strong CYP2D6 inhibitor (e.g., paroxetine, bupropion, or fluoxetine), the maximum dosage of deutetrabenazine was 42 mg/d (21 mg twice daily).
The switch cohort included participants with chorea in HD who enrolled in ARC-HD de novo and had been on a stable dosage of tetrabenazine with therapeutic benefit (although the benefit may have been suboptimal) for ≥ 8 weeks. These participants were converted overnight from tetrabenazine to deutetrabenazine. Initial deutetrabenazine dosages were calculated with a protocol-specified algorithm hypothesized to provide comparable systemic exposure to their previous stable tetrabenazine dosage [15, 16]. Participants in the switch cohort remained on their initial deutetrabenazine dosages for 1 week, after which dose adjustments could be made up to week 4, with an extended dose-adjustment period up to week 8. Similar to the rollover cohort, weekly adjustments (up or down) in increments of 6 mg/d up to 48 mg/d and of 6 or 12 mg/d up to 72 mg/d were permitted. For both cohorts, the stable-dose period was defined as week 8 through the last dose of study drug.
2.2 Safety Assessments
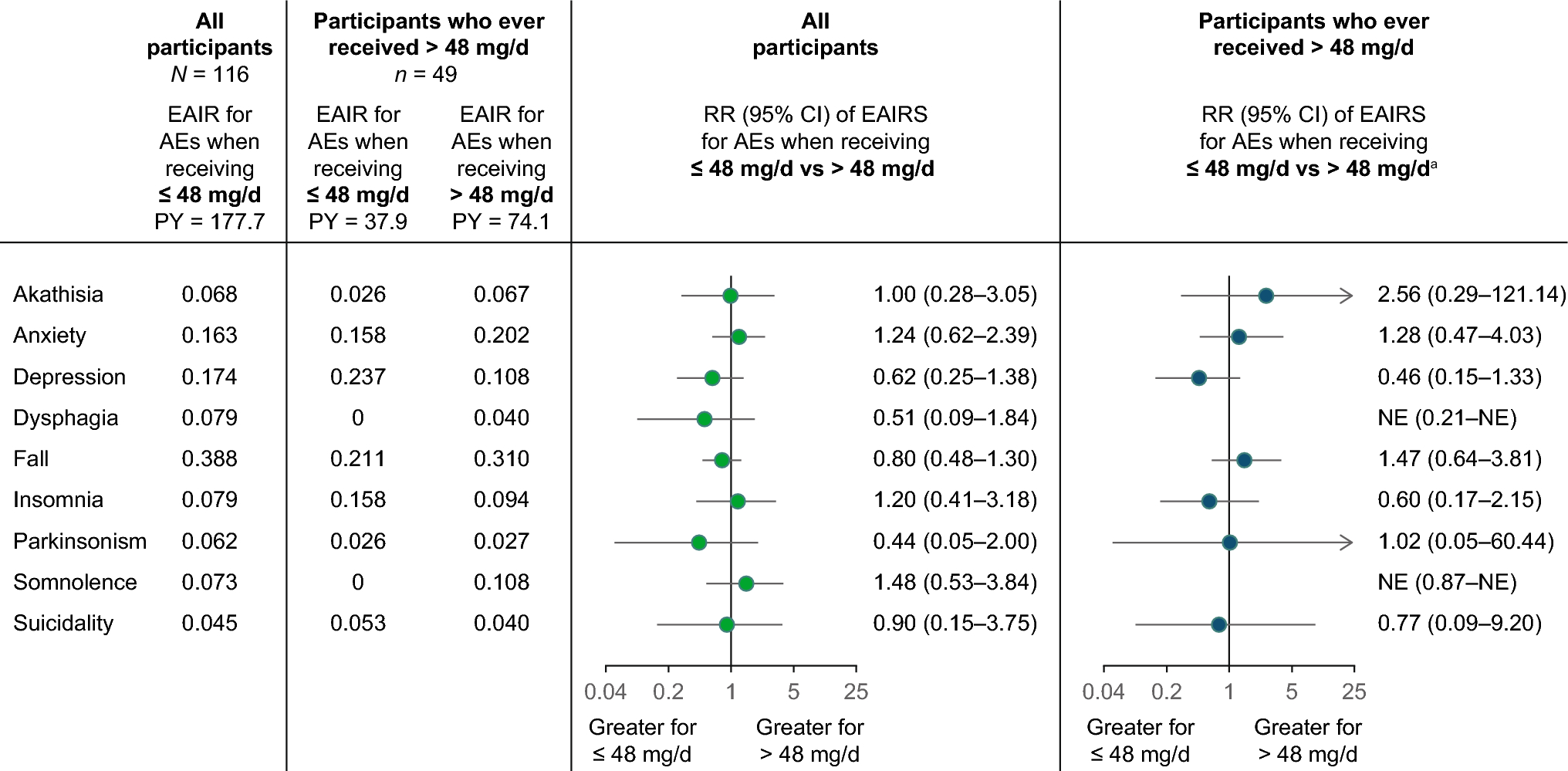
Safety and tolerability were assessed during in-clinic study visits and telephone study visits from the time informed consent was received through the end of follow-up (4 weeks after last dose of study drug) [15]. For this post hoc analysis, adverse events (AEs) of interest were evaluated using the following groupings of preferred terms: akathisia (including akathisia, hyperkinesia, psychomotor hyperactivity, restlessness, and agitation [preferred terms]), parkinsonism (including akinesia, bradykinesia, cogwheel rigidity, freezing phenomenon, hypertonia, masked facies, muscle rigidity, on and off phenomenon, parkinsonian crisis, parkinsonian gait, parkinsonian rest tremor, parkinsonism, Parkinson disease, and resting tremor [preferred terms]), fall, dysphagia (including aphagia and dysphagia [preferred terms]), somnolence, insomnia, anxiety, depression (including all preferred terms containing “depression”), and suicidality (including completed suicide, suicidal depression, intentional overdose, intentional self-injury, deliberate poisoning, self-injurious ideation, suicidal behavior, suicidal ideation, and suicide attempt [preferred terms]). Participant data (from both cohorts) were divided into two sets according to daily dosage: all participants, and participants who ever received dosages > 48 mg/d during the stable-dose period. AEs of interest reported during the stable-dose period (where dosages > 48 mg/d would be expected) were analyzed according to daily dosage (≤ 48 mg/d and > 48 mg/d) at the time of the AE report. Additionally, the temporal relationships (if any) between AE reports and dosage increases for participants who had dosage increases > 6 mg/d (at the discretion of the investigator) were evaluated.
2.3 Efficacy Assessments
In ARC-HD, changes in TMC and TMS scores from baseline to week 8 (titration period) and during the stable-dose period were evaluated [15]. Because baseline observations for participants who switched overnight from tetrabenazine to deutetrabenazine (switch cohort) were made while the participants were on different stable dosages of tetrabenazine, post hoc efficacy analyses were performed separately for the rollover and switch cohorts for the entire study period (titration and stable-dose periods). The lowest dosage needed for a TMC response (defined as ≥ 30% improvement from baseline in TMC score) was determined and plotted against baseline TMC score. Additionally, for each dosage level, the number of participants for whom that dosage was the lowest dosage sufficient to elicit a TMC response during the entire study period was assessed, and the cumulative proportions of participants who achieved a TMC response, by dose, were calculated. These analyses were also performed for participants with baseline TMC scores above and below the median value to determine whether there was a relationship between baseline TMC score and the dosage needed to achieve a TMC response.
2.4 Statistical Analysis
Exposure-adjusted incidence rates (EAIRs) for AEs reported during the stable-dose period (starting at visit 4/week 8) were used for analysis. EAIRs were calculated as the ratio of the number of individuals with the given AE divided by the total exposure time up to the end of follow-up (AEs per person-year) [17]. Comparisons between dosages are summarized as rate ratio (95% CI). The 95% CIs were calculated separately for each AE, assuming a uniform Poisson rate among participants while receiving the lower deutetrabenazine dosage and a different rate while receiving the higher dosage. Only participants who had baseline and post-baseline TMC scores were included in the efficacy analyses.








留言 (0)