Adjustment after SCI
The majority of adults with SCI, perhaps as high as 60%, cope and adjust well over time after their injury and its associated impairment, even though they face substantial daily challenges [6]. The reality is that most people with SCI will experience difficulties that challenge their resilience [7,8,9]. Difficulties include debilitating conditions such as respiratory infection, bowel and bladder infection, chronic pain, pressure injuries, sexual dysfunction, and cardiovascular dysfunction such as autonomic dysreflexia [7, 8]. Due to its life-changing nature, SCI will influence every aspect of a person’s life, including psychosocial aspects, such as interpersonal relationships, where partners or family members of an adult with SCI are vulnerable to relationship conflicts and breakdown in the first 2-years post injury, with many experiencing elevated anxiety and depressive mood [10]. The following discussion will assist in better understanding the influence of psychosocial factors that can act as barriers or facilitators to adjustment [5]. Whatever one’s view of this area, I believe if psychosocial barriers are left unaddressed, then SCI management and rehabilitation outcomes will become more complex and costly, ultimately leading to decreased QoL and unacceptable restrictions in social re-integration [5, 6].
Definition of psychosocial
The term “psychosocial” has had a variety of definitions in the health professions [11]. Here, a brief definition is offered based on a more comprehensive definition [11]. The concept of “psychosocial” primarily involves a person’s attitudes and perceptions about their psychological, physical, social, environmental, and spiritual status. The definition assumes that a person’s perceptions influence their behaviour related to their social access and mobility, their interpersonal dynamics with family and social networks, their environment, and wider society structures like education, culture, religion, and legal systems [11]. A definition of “psychosocial” also incorporates the idea that some factors (e.g. age, disability, physical health, material resources, and social support at the individual or social level) may improve or lower the psychosocial health of an individual [11]. Finally, “psychosocial” involves the dimension of time, in which its influence on health will vary over time, dependent on how these factors influence the person, their context and how factors interact with each other. For example, increasing age and presence of secondary conditions like pain, will more than likely be associated with decreasing cognitive capacity [5]. This definition of “psychosocial” will be applied in the ensuing discussion on factors that impact adjustment dynamics and will be applied when discussing a multifactorial model of adjustment dynamics.
Psychosocial impacts after SCI
There are many psychosocial factors that affect adjustment dynamics after SCI [5, 6, 12]. Research has consistently shown that adjustment after SCI is not only influenced by level and completeness of the injury and presence of physical co-morbidities, but also by psychosocial elements [5, 6, 9, 12]. For example, in a study examining resilience after SCI, psychosocial factors like self-efficacy were found to contribute significantly to resilience, whereas injury and demographic factors did not contribute significantly 12-months post SCI [13]. A recent narrative review focused on the adverse impact of psychosocial factors after SCI, focussing on relationships and family, finances and employment, the person’s living environment, community reintegration and sexual health, using the framework of the biopsychosocial model [12]. Readers are directed to this interesting paper for more detail [12]. In this paper, I examine five additional psychosocial factors which can act as significant barriers to adjustment. Much of this evidence has originated from my research. These factors include psychological distress, cognitive impairment, pain catastrophizing, sleep disorder and fatigue.
Psychological distress
The majority of adults who sustain a SCI, perhaps as high as 60–70%, will cope and adjust suitably, despite the challenges associated with this severe injury and lifelong disability [6, 13]. Nonetheless, most, if not all people with a SCI will initially experience grief and significant sadness as a consequence of the injury, which, though distressing, is considered an adaptive reaction to SCI [14]. Worryingly, evidence suggests that up to 40% are at risk of experiencing difficulties with sub-clinical or clinically elevated psychological distress and mental health disorder [5, 6, 9, 15, 16]. Results from a meta-analysis confirmed that psychological distress is clinically elevated after a SCI compared to able-bodied controls [15], with data indicating that distress had only begun to reduce 10 years post SCI [15]. A further meta-analysis investigated the prevalence of depression after SCI and concluded that around 26% of adults with SCI met a diagnosis of probable depression depending on the time post-injury [16]. Rates of post-traumatic stress disorder and anxiety disorders in adults with SCI are also higher than community rates [9]. Research that employed gold standard psychiatric interviews for a diagnosis and which followed adults with SCI prospectively from the acute stage of the injury to 12-months post injury, concluded that up 30% met psychiatric criteria of any psychological disorder [9]. Psychosocial factors significantly contributed to the risk of elevated levels of psychological distress 12-months after the SCI, including lack of social support, no care partner, catastrophizing thinking, and chronic pain [9]. Premorbid psychological treatment was a very strong identifiable risk, with the odds of developing psychological distress 12-months post SCI almost 24 times greater than those for someone with no premorbid history of psychological distress [9]. The same study established that psychological co-morbidities are also high after SCI [9]. Around 10% of participants met psychiatric criteria for two psychological disorders and 3% met criteria for three psychological disorders [9]. Major depressive disorder and substance use disorder was the most common co-morbidity, followed by major depressive disorder and suicidality. About 4% had a co-morbid PTSD and /or generalized anxiety disorder with depression [9]. Rates of PTSD with co-morbid pain is higher in veterans who sustained a SCI while serving in the military [17]. Evidence suggests that most if not all psychosocial challenges will act to increase or decrease psychological distress depending on the person and their circumstances [5, 6, 12].
Cognitive impairment
Cognitive impairment is a prevalent secondary health condition after SCI [18, 19]. It has been estimated that 12-months after the injury, the odds of an adult with SCI having cognitive impairment was about 18 times greater than that for someone without SCI [19]. Prospective research found that executive function, attention, perceptual (visuospatial), memory (learning), and language domains were all significantly reduced compared to an able-bodied control group [19]. However, a recent network meta-analysis concluded that deficits in cognitive function after SCI mostly occurred in the attention and executive function domains, while language and perceptual domains were least affected [18]. The presence of cognitive impairment in adults assessed in the acute and rehabilitation phase after SCI can have increased risk of adverse impacts on their mental health after discharge from hospital, when transitioning into the community, a time when personal resources will be challenged [19]. Without the comprehensive support provided during inpatient SCI care, those people with cognitive impairment will be more likely to believe their disability is beyond their control and feel helpless about their disability, making them vulnerable to poor self-management and associated secondary health conditions like infection, depression and clinically elevated anxiety [5].
Many factors can contribute to the development of mild cognitive impairment after SCI [19]. Traumatic brain injury (TBI) if comorbid with the SCI, can be associated with cognitive impairment [19]. Other factors that can contribute to cognitive impairment after a SCI include pre-morbid brain trauma and learning difficulties, fatigue, sleep disorder, chronic pain, elevated anxiety and depression, polypharmacy, substance abuse, older age and post-traumatic inflammation [19]. Treatments investigated for improving cognitive impairment after SCI are in their infancy, so this is a challenge for future work [20].
Pain catastrophizing
Chronic pain after SCI is commonly associated with other comorbid psychosocial conditions like fatigue, depression and functional limitations [5], and is also commonly associated with cognitive biases like pain catastrophizing and low self-efficacy in people with SCI [5, 21]. Pain catastrophizing involves negative cognitive appraisals including feeling helpless and overwhelmed, intrusive and repetitive negative thinking called rumination, and magnifying their fears, thinking how horrible and disastrous their life is [5, 21]. Pain catastrophizing can be a serious barrier to adjustment after SCI [5] and it will interact with other psychosocial factors to worsen outcomes, like low self-efficacy, the social environment, sleep disorder, excessive daytime sleepiness, fatigue and psychological distress [5, 21]. In prospective research following adults with SCI from rehabilitation and into the community 12-months after the injury, pain catastrophizing increased substantially in those with clinically elevated mood states during rehabilitation, while in those with normal mood, pain catastrophizing did not alter significantly over this time period.
This finding supports a multifactorial model that predicts that depressive mood will act as a moderator on catastrophizing [21]. This is clinically relevant because adults with SCI who are depressive have a higher risk of catastrophizing about their pain and our data also showed that these people will have higher levels of pain intensity [21]. This prospective data also indicated that the social environment into which the adults with SCI were discharged can exert an adverse impact, resulting in increased pain intensity and catastrophizing [21]. When adults with SCI are discharged into the community following their intensive rehabilitation, they of course will receive less professional support and assistance from the MDT, and consequently, their resources required to adjust will be challenged and they will often feel stressed and overwhelmed. It is crucial this barrier to the adjustment process be addressed by investigating effective counter-cognitive management strategies for strengthening self-appraisals and coping skills [5, 21].
Sleep disorder
Sleep disturbance such as obstructive sleep apnea can be a significant barrier to adjustment after SCI [5, 22]. Poor sleep quality has been strongly associated with other psychosocial problems like negative emotional wellbeing and low vitality, higher rates of unemployment, and greater problems with participation in people with SCI [22]. A related barrier is excessive daytime sleepiness, described as a susceptibility to falling asleep during the day [23]. Sleep disorder and excessive daytime sleepiness will diminish QoL and social participation, especially in those with cervical and thoracic lesions and sensorimotor complete injuries [5, 23]. Chronic pain can significantly disrupt sleep quality, and conversely, poor sleep can exacerbate levels of pain [23]. It has been argued that inadequate sleep and accompanying sleepiness will reduce top-down cortical/cognitive resources (e.g. attention), leading to decreased capacity to manage pain, and increasing risks of psychological distress [21, 23]. I recently examined the influence of pain catastrophizing on the ability of adults with SCI to stay awake during a behavioural test of daytime sleepiness called the Oxford Sleep Resistance Test [23]. If high pain catastrophizing was present, sleepiness was severely affected, with 70% of participants with SCI falling asleep, compared to 33% falling asleep for those with minimal catastrophizing [23]. Findings suggest significant sleep benefits may occur in adults with SCI by treating cognitive biases like catastrophizing, as well as addressing associated factors like fatigue, pain interference, low mood, and so on. This study again demonstrates how psychosocial factors can interact to créate even more problematic barriers to adjustment [23].
Fatigue
Chronic fatigue is another debilitating problem after SCI [5, 24]. It is a multifactorial condition that can be defined as excessive chronic tiredness involving feelings of physical and mental exhaustion and negative emotions, such as anxiety and poor mood [5, 24]. Major problems associated with fatigue can include increased chances of errors when performing tasks, reduced motivation, circadian rhythm disruption, and increased risk of anxiety and confusion [24]. In a controlled experimental condition requiring mental concentration over a period of 2–3 h, adults with SCI and able-bodied controls were compared for the extent that they experienced significant tiredness [24]. While the able-bodied participants experienced some tiredness, they did not reach extreme levels of fatigue, while 56% of the SCI participants experienced serious fatigue [24]. Psychosocial factors found to contribute to the development of fatigue consisted of poor self-efficacy and depressive mood [24]. Many people who sustain a SCI are of working age and employed at the time of their injury, so re-engagement in employment is an important goal of SCI rehabilitation and functional recovery. Re-employment can be associated with improved functioning, adjustment, self-esteem, wellbeing, financial independence and social integration, leading to higher QoL [24]. However, rates of employment remain low after SCI and psychosocial factors like fatigue interacting with other psychosocial barriers, will have a major impact on their ability to return to work [24].
A unified SCI rehabilitation management framework
I have endeavoured to illustrate how the above five psychosocial factors impact adjustment after SCI, and how they can interact to create barriers to positive adjustment. It is important now to consider a framework that incorporates such impacts and interactions. The Biopsychosocial Model of care provides a unified rehabilitation management framework for SCI rehabilitation, especially when delivered within the context of a PCC approach [4, 5]. Such a model views a person’s rehabilitation, health and well-being as the outcome of interacting physical, psychological, and social domains, where psychosocial domains of intervention are equally important as the physiological and medical domains [4, 5]. Each domain is necessary and is expected to play a critical role in helping the person to adjust and thrive [5, 13]. It is my belief that SCI rehabilitation delivered in such an atmosphere will optimize and enhance adjustment and resilience. SCI rehabilitation professionals in the SCI MDT have an exceptional opportunity to provide not only the best physical rehabilitation, but also optimal guidance through improving psychosocial health in their patients, which will continue to benefit them after discharge into the community [5, 6, 9, 13, 19, 21].
Like anyone, individuals with SCI must adapt continuously throughout their lives, and when faced with barriers, they need to adjust to maintain balance across the biopsychosocial domains mentioned above [5]. Rehabilitation will help them adjust to the multiple challenges they face. This introduces the necessity of viewing adjustment through a multifactorial model lens in which adjustment will be affected by multiple factors, including personal, social, environmental and illness specific factors, all of which can interact with the severity of the SCI and change in social roles, as well as life stressors (present and future), with consequent effects on wellbeing [5]. It is accepted that any attempt to describe the complex process of adjustment using a model format will, by definition, simplify the process [5], and it is important to factor this limitation into any SCI adjustment analyses or assessments.
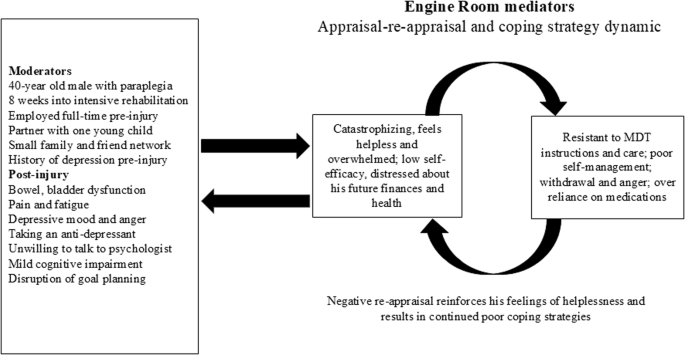
The spinal cord adjustment model
The Spinal Cord Adjustment Model (SCIAM) views adjustment after SCI as a multi-factorial, non-linear dynamic of adjustment over time [5,




留言 (0)