Setting
The VSCS is the primary care centre for people with spinal cord injuries in Victoria, Australia.
Study design and participants
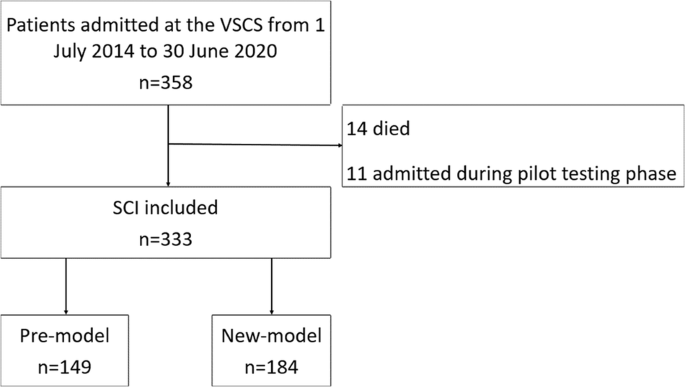
A registry-based cohort study of people with SCI managed before or after the introduction of the new model of bladder management care at the VSCS was conducted. Adult (>15 years) cases of traumatic SCI with a date of injury from 1 July 2014 to 30 June 2020, and acute admission managed at the VSCS, were included. The research was conducted in compliance with the National Health and Medical Research Council of Australia’s 2023 National Statement on Ethical Conduct in Human Research. Ethics approval for this study was granted by the Austin Health Human Research Ethics Committee (Project ID 78300) and the Monash University Human Research Ethics Committee (Project ID 29749). The research was conducted with approval of a waiver of consent as existing data were used.
Procedures
Eligible cases were identified using the VSTR, the State’s population-based registry for major trauma. Data extracted from the registry included demographic information, cause (transport, fall or other) and intent of injury (intentional, unintentional, intent cannot be determined), pre-existing conditions (Charlson Comorbidity Index), nature of the SCI, the Injury Severity Score (ISS), management in the State’s trauma system (managed at the VSCS or other trauma service, inter-hospital transfer status, intensive care unit admission status), in-hospital outcomes source of funding for the admission. Data related to readmission, hospitalization and ED presentation were extracted from the Austin Health electronic medical record (EMR).
The Charlson Comorbidity Index (CCI) is used to measure mortality risk and burden of disease [19, 20]. It can be used to prognosticate patient long-term mortality [20]. The quintile of socioeconomic status was measured by applying the Index of Relative Socioeconomic Advantage and Disadvantage (IRSAD) to the patient’s postcode of residence. Range included 1 (most disadvantaged) to 5 (most advantaged) [21]. Remoteness of residence was assessed by applying the Accessibility/Remoteness Index of Australia (ARIA) which classifies the patient’s postcode of residence into 1 of 5 categories including major city, inner regional, outer regional, remove and very remote [22]. These categories were consolidated into 2 categories; major cities, and inner regional, outer regional and remote. UTI was defined using the ICD-10-AM diagnosis code, N39.0, for the admission or ED presentation.
Management strategies of bladder care included IDCs that were changed every 6 weeks. They were changed earlier if they became blocked or the patient was diagnosed with a UTI. No antibiotics were administered prior to routine changes [15, 23].
Intermittent catheterisation was completed by either the nursing staff or patient while in hospital. If completed by nursing staff a sterile technique was performed however if a patient completed the IC a clean technique was used. No catheters were re-used. Patients had the option to utilise a self-contained unit [11].
The outcomes of interest for this study included:
i.
Readmission (yes/no) and number of readmissions to hospital for UTI in the first 2 years post-injury.
ii.
ED presentation (yes/no) and number of subsequent presentations to ED for UTI in the first 2 years post-injury.
iii.
Hospitalisation (yes/no) and number of hospitalisations (ED or readmission) for UTI in the first 2 years post-injury.
The outcome of “hospitalisation” included both subsequent ED presentations and hospital readmissions at the Austin. For all analyses, ED presentations excluded the cases of hospital readmission that were via an ED; ED presentations were only where the person was managed and directly discharged from the Austin ED.
Statistical analysis
For analysis, change in the ‘pre’ model of care commenced 1 August 2017 and ended on 30 April 2017 to remove any potential confounding from early cases, where the new model of care was piloted, between 1 May and 30 July 2017. Frequencies and percentages were used to summarise categorical variables. Median values and interquartile range (IQR) or means with standard deviation (SD) were used to describe continuous data. Baseline variables were compared between model of care groups using t tests if continuous data were normally distributed, Mann–Whitney u tests for non-normally distributed continuous variables, and chi-square tests for categorical variables.
The number of readmissions to hospital, and presentations to ED, for UTI in the first 2 years post-injury were modelled using a negative binomial model to allow for the overdispersion in the data. The model was adjusted for differences in the case-mix on acute admission and an indicator variable created to account for the small proportion of cases where a full 2 years of follow-up had not yet been reached (n = 16). Adjusted incidence ratios (IRR) along with the corresponding 95% confidence intervals (CI) were reported. All analyses were performed using Stata Version 17. A p-value < 0.05 was considered significant.




留言 (0)