
記住我




The eMOM pilot study was a combination of a crossover and a parallel study design, starting after randomization with a two-week crossover phase (short-term effects). This was followed by a parallel randomized controlled trial (RCT) which continued until delivery (long-term effects). The short-term effects of the crossover have been reported previously [37]. The focus of this article is on the long-term effects (up to delivery) of the intervention on maternal and newborn outcomes.
Participants and allocationThe participants were recruited from Helsinki and capital area in Finland between December 2018 and March 2020 via the municipal outpatient maternal health clinics, where pregnant women are offered free maternal healthcare. The last participant completed the study in June 2020.
Inclusion criteria for study participation were clinical diagnosis of GDM (either one of ≥ 5.3 mmol/L fasting blood glucose or ≥ 10.0 mmol/L at one hour, or ≥ 8.6 mmol/L at two hours past an oral glucose tolerance test (OGTT) of 75 g glucose), having a singleton pregnancy, gestational week (GW) up to 29 at the recruitment and not using any medication that influence glucose or cholesterol metabolism (e.g. oral corticosteroids).
Women were excluded from participation if the diabetes diagnosis was either T1D or T2D, were unable to follow the diet protocol due to dietary restrictions (e.g., allergy), of other than European descent (themselves or child’s father), or if they had other issues that would interfere with participation (e.g., inadequate Finnish language skills or substance abuse).
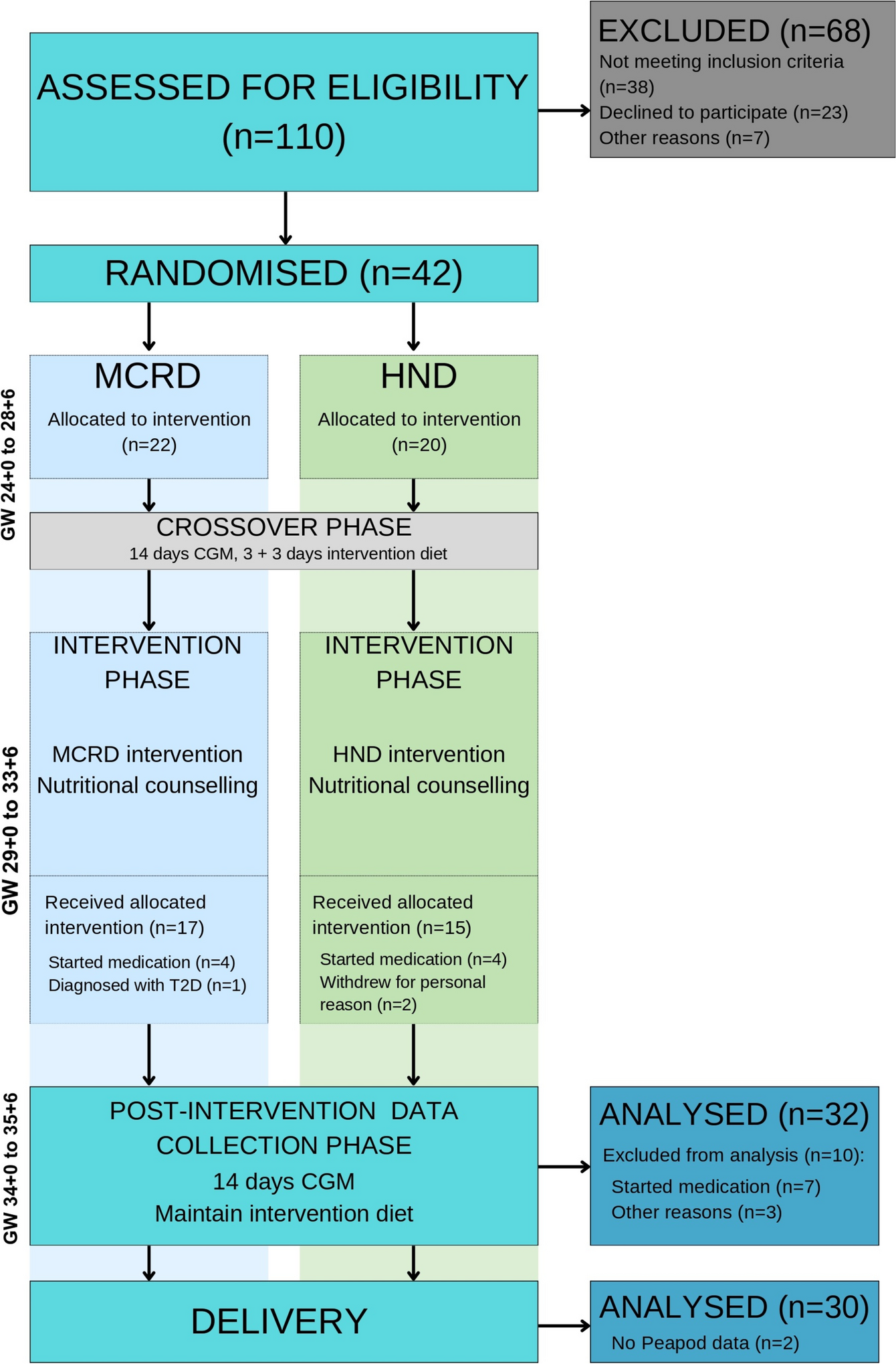
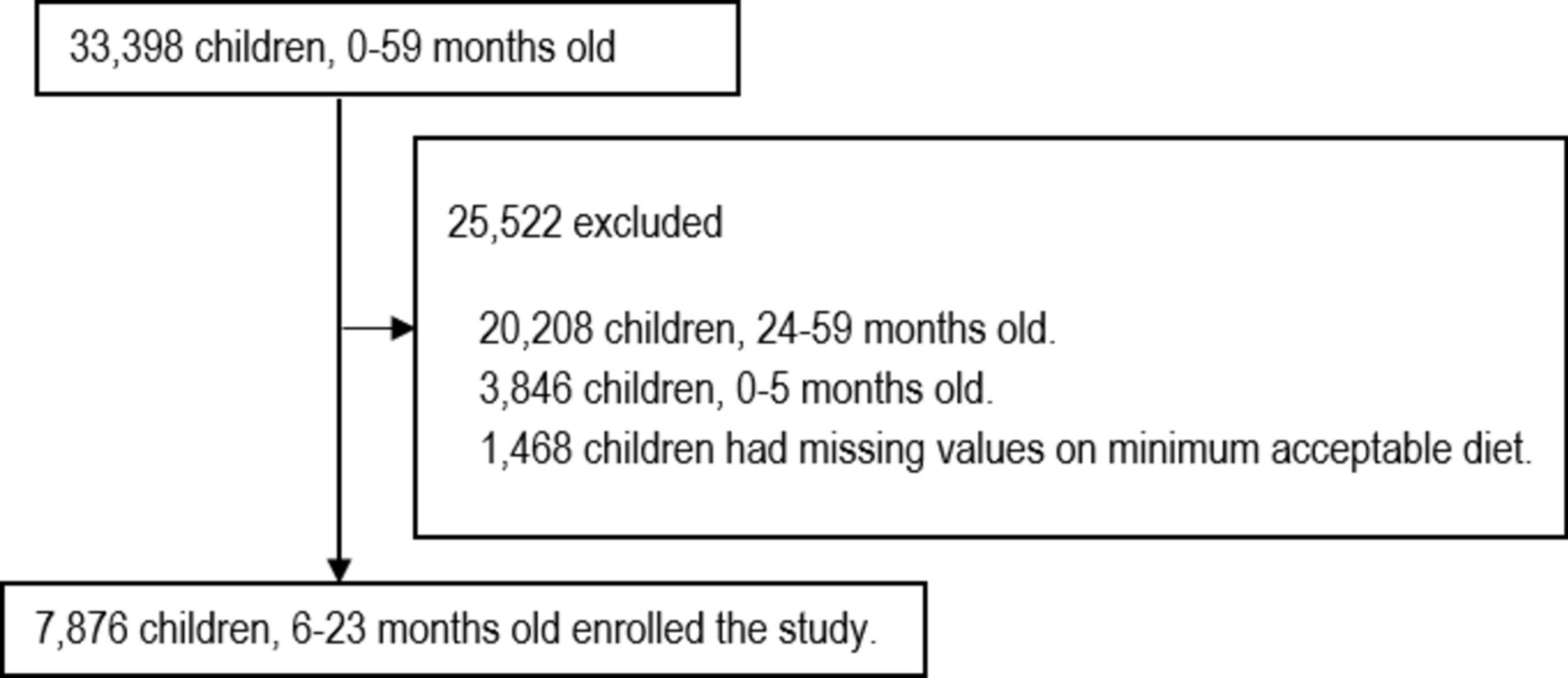
A total of 42 women were recruited to start the intervention in this pilot study (Fig. 1). A randomization with blocks of four (body mass index, BMI, above/below 30 kg/m2 and nulli-/ primi- & multipara) was computer assisted in advance. Details of allocation and recruitment have been described previously [37]. Participation in the study was discontinued if a participant was prescribed pharmacological treatment (metformin or insulin).
Fig. 1
CONSORT flow chat. MCRD: Moderately carbohydrate-restricted diet. HND: Healthy Nordic diet. CGM: continuous glucose monitoring. GW: gestational week
The study personnel and participants were not blinded for diet allocation during the study as it was deemed impossible considering the setting of the study.
InterventionsDiet protocolsThe participants were first introduced to both diet protocols during the crossover phase of the study (as described in [37] and continued to follow their most recently assigned intervention diet immediately after the completion of the crossover. The baseline visit with a study nurse occurred in GW 24 + 0 to 28 + 6, and the intervention diet was followed until the end of the pregnancy.
The diet recommendation for GDM treatment in Finland [19] was the basis for the MCRD (Table 1). The MCRD was characterised by a moderate reduction of carbohydrate (~ 40 E%), and otherwise followed the food-based guidelines of the Nordic Nutrition recommendations. The HND intervention was characterised by preference for Nordic foods, e.g., oats, barley and rye as grain sources and Nordic fruits and berries. The vegetable, fruit and berry recommendation were 1 kg/day. Further, the instructions were to prefer plant-based protein sources (e.g., legumes and industrially produced plant-based products high in protein). Energy requirements for both diets were estimated using the Nordic Nutrition Recommendations [38] for pregnancy. Participants were not required to monitor energy intake as the diets were not intended to be isocaloric for this pilot study.
Table 1 Description of the intervention diet protocols. Energy intake estimation, macronutrient target and food group specificationsNutritional counsellingBoth groups received individual nutritional counselling tailored to support the participants in their allocated diet protocol. The counselling sessions consisted of three face-to-face sessions and two phone calls (Fig. 2). In addition, the participants had the possibility to communicate with the nutritionist via WhatsApp chats at any time. The nutritionist also communicated once or twice weekly to the participant via WhatsApp by posting inspirational recipes, links to articles and tips for exercise and relaxation. Educational materials were prepared by the eMOM nutritionists in the form of three educational booklets that were handed out at each of the face-to-face consultations. They were aimed to provide information on food choices, health behaviours that influence glycaemic control and give recipe inspiration. Additional information about healthy lifestyles beyond pregnancy and the importance of breastfeeding was included in the last booklet. One of the pamphlets also included an example 15-min home-exercise routine designed to be suitable for any level of fitness, and a general advice about aiming for daily 30 min daily or 150 min weekly of moderate-intensity physical activity (PA) e.g., brisk walking [39]. The educational material covering postpartum health, breastfeeding, and physical activity was the same for both groups.
Fig. 2
The participant journey, schedule and timeline of the eMOM study. CGM: continuous glucose monitoring
The first face-to-face consultation lasted approximately 2 h and consisted of a dietary anamnesis and detailed instructions about the allocated intervention diet. The remaining consultations were approximately 60 to 90 min each, while the phone calls were 15 to 20 min each. The main topics of the face-to-face consultations followed the contents of the session-designated educational booklet. The nutritionist practiced with reflective listening and supported the participants to modify their allocated diets taking into account their background and preferences while staying within the intervention protocol. Personalised mini-goals for diet changes followed the SMART-goals principles (Specific, Measurable, Achievable, Relevant and Time specific) to promote lasting changes [40]. Achievements of the goals were monitored through self-reflection and assisted by motivational interviewing [41] by the nutritionist. The content of the phone calls included participant support and dietary advice if needed.
Food incentivesAll participants received a bag of food in each of the face-to-face consultations with ingredients to one recipe from the educational booklet. This food bag also contained other products, that were suitable for the intervention diets. To assure that all participants took the recommended daily dose of vitamin D [42] all participants received vitamin D supplements (10 µg/day) to last the duration of the entire trial period.
Data collection and preparationContinuous glucose monitoring (CGM, Freestyle Libre®, Abbott, USA) measured the primary outcome of this study, %TIR, worn during a 2-week period in the 3rd trimester of pregnancy (GW 34 + 0 to 35 + 6).
Secondary outcomes were other blood parameters related to glucose, insulin and lipid metabolism, maternal nutrient and food intake, and neonatal body composition. Please see: Continuous glucose monitoring, Blood samples, Food diaries, Physical activity Accelerometers, and Newborn body composition.
Continuous glucose monitoringThe CGM sensor (Freestyle Libre® 14-day system, Abbott, USA) was worn for 14 days on GW 34 + 0—35 + 6. All sensor -related procedures and data management were performed according to manufacturer’s instructions. The Freestyle Libre ® sensor was attached to the participants’ upper arm, and coupled with a hand-held reader, which showed the current tissue glucose concentration, a glucose curve of the last 8 h and glucose measurement history. The sensor measures glucose concentration every minute, and the measurements are stored in a frequency of 15 min. Due to limited memory capacity of the sensor (maximum 8 h of data), the participants were instructed to scan the reader at least once during the daytime, before going to bed, and first thing in the morning. CGM glucose data was collected for the full duration of the 14 days. To limit inaccurate reading in the sensor adjustment period, we excluded the first 72 h of the data from analysis. The first measurement day of the CGM data included in the analysis was defined as starting at 00:00 and the last measurement day ended at 23:59. Data quality was ensured by checking the number of glucose observations, expecting each 24 h time period to contain at minimum 96 observations (automatically scanned by the sensor) times 11 days of CGM data (= 1056 observations). Participants with over 20% missing data had their glucose curves inspected individually and decided on a case-by-case basis whether the glucose data held a satisfactory data quality [43]. One participant had missing data for four days (~ 35% missing) and was excluded from all CGM related analyses. Other participants with any missing CGM data were a result of occasional infrequent sensor scans (e.g., slept longer than 8 h), and none of these participants had > 11.5% missing data. TIR was defined as a percentage of the total sensor time [number of measurements ≤ 7.8 mmol/l divided by the total number of measurements] for each participant. Measures of glucose variability, i.e., mean sensor glucose, sensor standard deviation (SD), the coefficient of variation [sensor SD divided by the mean sensor glucose] (CV), minimum and maximum glucose values were calculated from CGM data for each participant.
Blood samplesFasting (10–12 h) blood samples were collected in conjunction with the study visit at baseline and the study visit in GW 34 + 0. The detailed protocol for blood sampling and analysis has been explained elsewhere [44]. Samples were analysed for glucose metabolism (plasma glucose and insulin), blood lipids (total cholesterol; high-density lipoprotein, HDL; and low-density lipoprotein, LDL; triglycerides, TG), alanine aminotransferase (ALAT), HbA1cand high-sensitive C-reactive protein (hs-CRP). Homeostatic model assessment of insulin resistance (HOMA-IR) value was calculated from fasting insulin and glucose using the following formula [fasting insulin (mU/L) × fasting glucose (mmol/L)/22.5]. Homeostatic model assessment for beta cell function (HOMA β) was calculated by using the formula [20 × fasting insulin (mU/L)/fasting glucose (mmol/L) – 3.5] [45].
Food diariesAll participants recorded all food and beverage items and their amounts consumed for three consecutive days in a food diary. We analysed two food diaries: filled at baseline (prior to intervention start), and at GW 34. The participants were instructed to include brand names, and consumed amounts in household measures such as a tablespoon, a cup, a scoop, or in weight units, if available. For quality assurance, the food diaries were checked upon return by the nutritionist and, if necessary, supplemented by a short interview. The food record data were entered into a nutrition calculation software (AivoDiet, v. 2.2.0.1. Aivo Finland OY, Finland). All data from the food diary, both at the nutrient level and the food ingredient level were analysed as a three-day average consumption in grams. The food intake was categorized into food groups based on their nutritional content (e.g., dairy, fermented dairy, seafood and meat). For the food level analysis, only relevant categories in terms of the intervention contents were extracted (see Table 1). The food data categorization was performed in AivoDiet (AivoDiet, v. 2.2.0.1. Aivo Finland OY, Finland).
Physical activity accelerometryParticipants wore an accelerometer (UKK RM42, UKK Terveyspalvelut Oy, Tampere, Finland) at the hip during waking hours, excluding shower and activity in water. The device was also worn on the non-dominant wrist during sleep. Movement intensity and body posture data were converted to metabolic equivalents (MET, one MET = 3.5 ml/kg/min of oxygen consumption) from raw data according to [46]. Light physical activity (LPA) was classified as ranging from 1.5 to 3.0 METs and moderate-to-vigorous physical activity (MVPA) was classified as METs exceeding 3.0. Lower intensities were categorized as sedentary behaviour (SB) or standing (< 1.5 METs). For one day of accelerometer data to be accepted for analysis, it needed > 10 h of hip-worn data.
Newborn body compositionThe neonates body composition (fat mass, fat-free mass and percentage of body fat) was measured by air displacement plethysmography with the PEA POD® (COSMED, USA) within the first two days after birth. The measurement was performed twice, and in the case of fat percentage difference > 2% between the two measurements, it was repeated a third time. The average of two measurements closest to each other was used for data analysis [47]. The newborn body fat percentage was calculated [fat mass (g) divided by sum of fat mass (g) and fat-free mass (g) multiplied by 100]. The Z-score of birthweight was calculated based on representative Finnish data from Sankilampi et al. [48]. A birthweight of ≥ 4000 g was defined as the threshold for macrosomia. Small-for-gestational age (SGA) was defined as < 10% percentile of the Z-score, and large-for-gestational age (LGA) was defined as > 90% percentile of the Z-score.
QuestionnairesThe participants were inquired about their demographic data, health behaviors, and PA at baseline. Height and pre-pregnancy weight were copied from the maternal health clinic record, while weight were measured at study visits [37].
Statistical analysisAll numerical data underwent thorough quality check (i.e., outliers), and correction of unusual or missing values when possible. All laboratory blood test results were entered to the database as double entries to facilitate identification of typing errors. BMI was calculated by [weight in kilograms/height in meters squared]. Delta variables (Δ) were created [post-intervention value minus baseline value] to analyze postintervention changes for food consumption, macronutrient consumption, blood test results and HOMA indices.
CGM data was analysed for between-group differences post intervention, while diet (macronutrients and consumption of food groups) and blood sample data were analysed for between-group differences in changes from baseline. Due to small sample size the newborns body composition, birthweight and -length were compared between the groups with both genders pooled together. Groups were compared by two-sided t-test or Wilcoxon test with continuity correction depending on the data distribution. Chi-square and Fisher’s exact test was used to analyse categorical data. As an exploratory analysis, a pooled correlation analysis (all participants) of maternal factors, glucose control, intake of macronutrients, consumption of select food groups and newborn body composition measures (fat-free mass, and bodyfat percentage) were performed to investigate whether dietary factors had influence on glycemia or newborn outcomes. Pearson’s R and Spearman’s Rho methods were used.
No power calculation was made for this pilot study. All statistical analyses were performed with R programming language (version 4.0.5, The R Foundation for Statistical Computing, Austria. URL: https://www.R-project.org/) in RStudio (2023.06.2 “Mountain Hydrangea” release, RStudio: Integrated Development for R. RStudio, PBC, USA. URL: http://www.rstudio.com/).
留言 (0)