Introduction
2025 will be a year of change for the healthcare and life sciences industries. In medicines innovation, the dominance of specialty medicines, primarily in oncology, immunology and rare diseases, is being challenged by the rapid expansion in the use of new obesity medicines that address a broad range of cardiovascular and metabolic risk factors. While the financing available for investment and mergers and acquisitions looks promising, the ability to use innovative medicines is being hindered by capacity challenges in healthcare systems, and many are undergoing reform as a result. Across drug discovery and development, as well as in healthcare delivery, artificial intelligence (AI) is becoming increasingly widespread and empowering, and 2025 will see regulations on its application.
These changes are occurring in an increasingly unstable environment. Geopolitical friction is threatening the trend towards the globalization of life sciences, and the sector must navigate these uncertainties to ensure continued progress. Here, we highlight some of the key areas for progress in the coming year.
Oncology innovation
Oncology will remain at the forefront of therapeutic innovation. This year could see the FDA approval of the first personalized cancer vaccine, Moderna’s mRNA-4157 in combination with Merck & Co.’s PD1-targeted monoclonal antibody pembrolizumab (Keytruda) for melanoma — an approach that could transform cancer treatment. Impressive data for bispecific antibodies have recently been reported. In non-small-cell lung cancer, ivonescimab, which targets PD1 and VEGF, became the first agent to surpass pembrolizumab in a phase III trial. Although the data were from a trial conducted in China only, global studies of ivonescimab are ongoing, and a new standard of care could be in the offing. Zanidatamab, the first bispecific antibody to bind to two epitopes on the same target (HER2), was approved by the FDA for biliary tract cancer in November 2024, and is expected to reach patients this year.
Progress in the route of administration also continues. In September 2024, the FDA approved a formulation of the PDL1 inhibitor atezolizumab (Tecentriq; Roche) for subcutaneous injection, which was swiftly followed by an approval in December for a subcutaneous formulation of Bristol Myers Squibb’s PD1 inhibitor nivolumab (Opdivo). This could soon be joined on the market by a subcutaneous formulation of pembrolizumab, following its success in a phase III trial in 2024.
Obesity medicines
The global market for obesity prescription medicines was expected to exceed US$30 billion in 2024, driven by the rise of the GLP-1-based therapies Wegovy (semaglutide, Novo Nordisk) and Mounjaro/Zepbound (tirzepatide, Eli Lilly), which also targets the GIP receptor. Although no new agents are expected to launch in 2025, readouts on key trials of marketed and pipeline medicines are expected, including cardiovascular outcomes data for tirzepatide in patients with type 2 diabetes from a trial known as SURPASS-CVOT, and results from the EVOKE and EVOKE+ trials of oral semaglutide1, which are investigating its effects on cognition and function in patients with early-stage Alzheimer disease. Phase III data on new molecules include results for Lilly’s orforglipron, which could be the first oral GLP-1 receptor agonist to enter the market, and for the first potential competitor to the Novo Nordisk/Lilly duopoly: Boehringer Ingelheim’s survodutide (which targets the glucagon and GLP-1 receptors). Novo Nordisk’s CagriSema (which targets the amylin and calcitonin receptors in addition to the GLP-1 receptor) will also have an important head-to-head readout against tirzepatide.
Decisions made by payers about initiating or expanding coverage for obesity medicines will provide vital indicators for the longer-term development of the market. The biggest publicly funded coverage for obesity medicines globally is the US Medicare scheme for people aged 65 and over, with Wegovy covered for people with obesity and cardiovascular risk. However, the incoming US administration could oppose expanding coverage of such medicines, favouring non-pharmacological measures. In Europe, NHS England will embark on a major roll-out of Mounjaro, starting with people with a body mass index of 35 and over with at least one co-morbidity, with the expectation of expanding to treat at least 220,000 people in the next three years. This roll-out is being accompanied by a five-year real-world trial known as SURMOUNT-REAL that is expected to begin in 2025, reflecting the desire of healthcare payers to gather detailed evidence on the cost/benefit of obesity medicines. More real-world evidence for these medicines (mostly from private prescriptions) will emerge in 2025, including on patient compliance.
Investment and M&A outlook
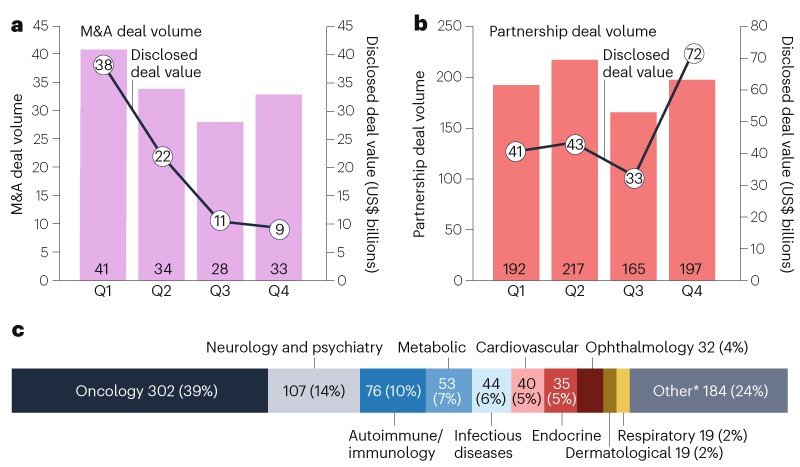
Following a rebound in 2023 from the lows during the pandemic, biopharma merger and acquisition (M&A) activity was more subdued in 2024, with aggregate deal value reaching $45 billion, down by 62% compared to the previous year. Although 2024 did not provide the catalysts to fuel M&A momentum, the drivers that support deal making continue to be strong heading into 2025.
On the demand side, deal capacity among big pharma companies exceeds $1.5 trillion, and more than $200 billion of revenue from marketed products will be exposed to loss of exclusivity by 2030, with up to 64% of some of big pharma’s current sales at risk. In addition, there is growing pressure from investors to engage in key growth areas, such as obesity, antibody–drug conjugates and bispecific antibodies.
On the supply side, biotech companies are developing ~70% of the clinical-stage pipeline, with 60% of their assets unpartnered, including several sought-after obesity candidates supported by recent trial readouts, such as Viking’s dual GLP-1/GIP receptor agonist VK2735 and Structure Therapeutics' oral GLP-1 receptor agonist, GSBR-1290. Furthermore, despite a re-opening market for IPOs (initial public offerings) and biotech stocks being buoyed by falling interest rates, two-thirds of public biotech companies remain under-capitalized, probably with less than twelve months of cash runway.
The near-term outlook for M&As in 2025 remains cautious, as deal makers digest the outcomes of the US election and the direction of the macro-economic, geopolitical and regulatory environment, including potential amendments to the US Inflation Reduction Act. However, once the cloud of uncertainty begins to lift, we expect more bullish M&A activity, probably helped by a less activist Federal Trade Commission, as pressure mounts on big pharma companies to replenish upcoming revenue losses and close a widening growth gap.
A divergence in AI applications
The capabilities and applications of AI tools will continue their rapid growth. However, the complexity of predicting patient-level outcomes, coupled with incoming regulation in Europe, is expected to drive a divergence between the wide-ranging application of AI in preclinical drug development and a more incremental roll-out in clinical contexts.
The European Union’s AI Act has requirements that begin to apply from 2 February 2025 and will have regulatory implications for AI globally. For medicines development, the act will affect AI used in the clinical setting: to diagnose, monitor, support treatment decision-making or otherwise interact with patients. The only other regulatory superpower, the US, seems unlikely to go beyond its current approach or that of the EU.
Beyond regulation, the computational performance of AI should at least double within the next year, driven by steady progress in algorithmic efficiency, hardware efficiency and training data availability. This will improve its ability to make biological or medical predictions. However, biological systems are highly complex, and moving from predictions at the molecular level to those at the cellular or human-level is challenging. Therefore, we expect more AI-discovered molecules reaching clinical trials but a slower application of AI in clinical evidence generation.
Growing consumerization
Cardiometabolic conditions and other high-prevalence chronic diseases are seeing increasing consumerization, by which we mean growing willingness of people to pay for private consultations and the private prescription of medicines, a subsequent growth in private prescription platforms, and clinical-grade diagnostics and monitoring moving into the hands of the consumer. The heart monitoring and electrocardiogram functionalities of smartwatches are an example of this trend. This consumerism expands markets and raises ethical questions around equity of access to healthcare.
There are several drivers of this trend. Healthcare systems are facing a huge dual budget challenge as the rising impact of chronic conditions, such as obesity, comes with the cost of new treatments for them. In part due to this, these systems are restricting coverage, further fuelling the trend towards out-of-pocket payments and the devolution of treatment decisions to patients.
This trend is proceeding at different rates across countries, diseases and medicines, driven by other commercial factors: the time window for innovative therapies to recover development costs is becoming shorter, and requirements for real-world evidence to bolster a product’s value proposition are increasing, further strengthening the case for continuous patient engagement to create demand and ensure access.
Conclusion
This year will bring changes to the fundamentals of medicines development and the life sciences industry: a strengthening of AI and financial capacity will be counterbalanced by greater geopolitical friction, and the change in the US administration will affect the world’s largest pharmaceutical research base and market, and have global geopolitical ramifications that extend into medicines development.
Against this backdrop, progress in medicines innovation will largely correspond to areas of great unmet need, with most notable trial readouts and approval decisions expected for obesity, oncology, pain and rare diseases. As with other ecosystems, changes to the healthcare system will be subject to resistance and feedback loops — in this case healthcare system capacity constraints, regulation and new private markets.

留言 (0)