Summary of Main Findings
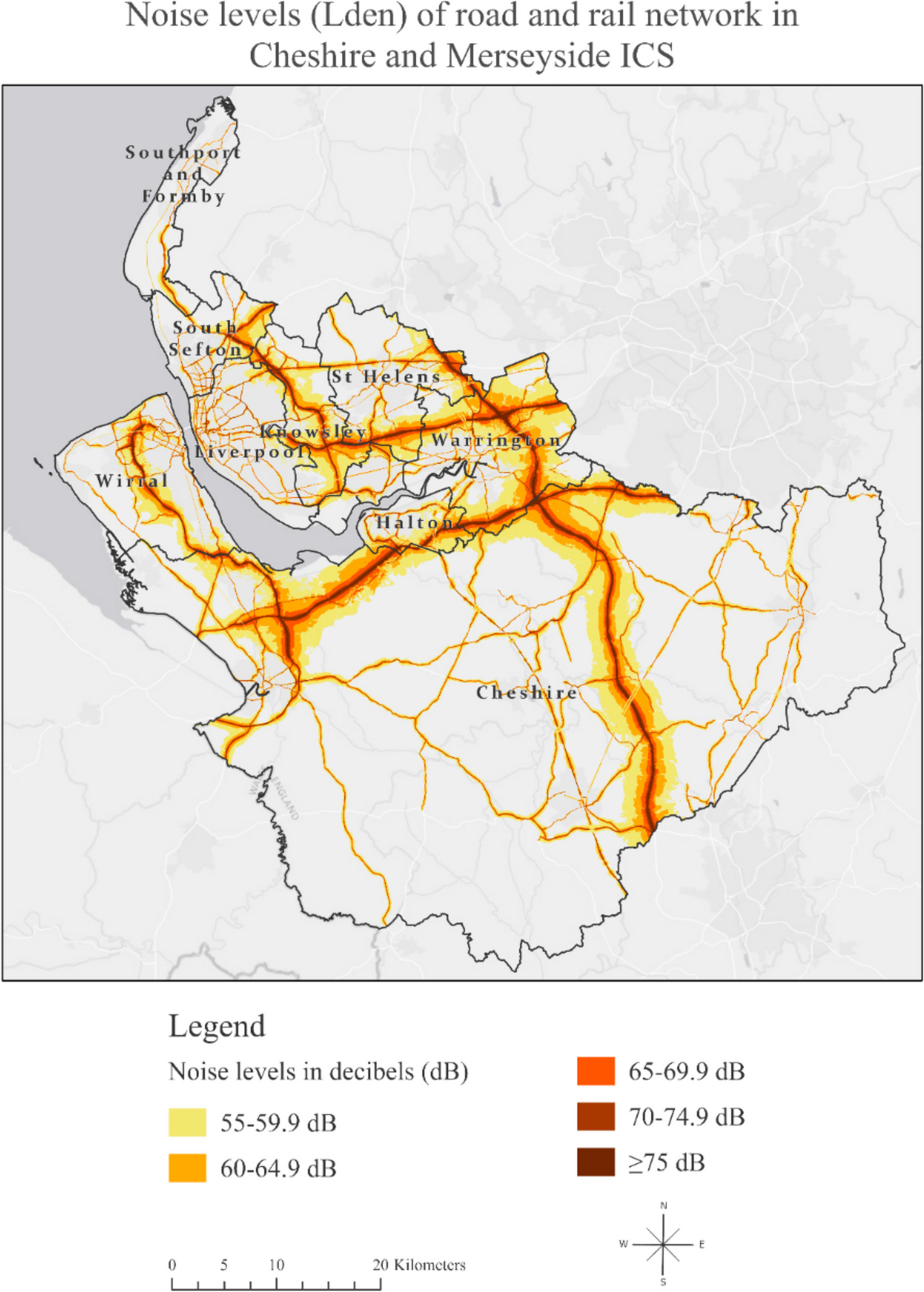
To the best of our knowledge, this is the first study to investigate the impact of transportation noise pollution on mental health in England. Our study identified areas with a heavier noise burden, offering the opportunity to tailor public health interventions in these regions to enhance the quality of life in urban environments. Combining transportation noise from road and rail networks, we found that Warrington and Knowsley had the highest percentage of noise coverage, with over half of their respective areas exposed to transportation noise exceeding 55 dB on a 24-h basis.
Our research revealed that, although transportation noise did not have an equal direct role in explaining depression levels in all areas, it did play a significant mediating role, amplifying the effect of other factors on depression, such as the impact of health deprivation and disability.
Comparison with Previous Literature
Environmental noise pollution has been associated, in general, with poor mental health indirectly [16,17,18], and the effects are varying from increased stress and anxiety levels [19, 20] to hyperactivity [21, 22], a decline of well-being [23], and an increase of psychotropic medication [24, 25].
Previous studies investigating explicitly the association between environmental noise pollution and depression have yielded conflicting research results and an incomplete overview of the effects of all noise sources on mental health. As suggested by the systematic review and meta-analysis by Hegewald et al. [26], which included 11 studies of road and 3 studies of railway traffic noise, there were indications of 2–3% increases in depression risk per 10 dB Lden [26]. Interestingly, a recent big data analysis using data from the UK Biobank found a negative association between moderate road traffic noise and major depression [27].
However, no previous study has examined local regression models to comprehend the varying relationships and spatial patterns, aiming to understand how local geographical factors influence the connections between variables, recognising that different places possess unique characteristics that impact these relationships. Moreover, although a US-based nationally representative survey explored the association between noise pollution and mental health in adolescents [28], no previous study has spatially examined the combined impact of road and rail noise on adults’ mental health, evaluating primary care records of depression as an outcome assessment.
Strengths and Limitations
Our paper has a significant strength by employing an innovative structural equation spatial modeling methodology in small geographical areas. This approach allows for the examination of multiple mediators and links in the spatial chain during the model testing process. Additionally, the GSESM analysis furnishes crucial information on model fit, gauging the consistency of the hypothesised mediational model with the data and establishing zero-order relationships among variables. Notably, this methodology, which has not been previously utilised in the literature, leverages recent advancements in computing power, opening up new possibilities for the analysis and modeling of spatial data [15, 29].
Our study, therefore, breaks new ground by exploring the link between environmental noise and the spatial epidemiology of depression using spatial analysis methods. This unique aspect forms a significant strength, particularly as no prior research has delved into this connection using spatial methodologies. This research contributes to the field by expanding the scope beyond earlier investigations limited to selected primary care practices [30]. Instead, our study encompasses the entirety of practices in the Cheshire and Merseyside Integrated Care System (ICS), analysing records from a substantial 2.7 million individuals. The application of spatial methodology empowers us to identify spatial clustering patterns, pinpoint localised hotspots, and discern specific local risk factors—accomplishments that traditional non-spatial regression models are not achieving.
However, it is crucial to acknowledge several limitations. The data on depression are reliant on the recording practices of general practitioners (GPs), introducing a potential source of bias. GPs’ decisions to diagnose depression may also be influenced by personal biases or preferences, as they might record symptoms instead of providing a formal diagnosis of depression [31]. Another constraint is that the Quality and Outcomes Framework (QOF) depression prevalence offers aggregate data for all adults without specific information on adolescents or distinct age groups, nor details on those in retirement status, potentially confounding the associations [32].
In our analyses, we were constrained to using the weighted 24-h indicator (Lden) that combines daytime and nighttime exposures from strategic noise mapping for rail and road noise [7] that was used in accordance with EU Directive 2002/49/EC [33]. From a mental health perspective, we believe the 24-h exposure metric serves as an effective annoyance-based indicator, reflecting cumulative noise exposure (WHO & Theakston Frank, 2011). Previous studies have utilised both weighted and non-weighted averages (Leq, Ldn, and Lden), and we acknowledge that peaks and troughs of noise may have distinct effects on mental states, particularly regarding sleep disturbances caused by sudden sounds, such as sirens in urban settings [34]. As noted by Basner et al. [35], undisturbed sleep is crucial for high daytime performance, well-being, and overall health. Unfortunately, we were unable to analyse peak noise levels with the available data. Further investigation into the differential impacts of daytime noise exposure in living areas versus nighttime exposure, as well as the effects of noise peaks and troughs, is warranted.
Research and Policy Implications
The findings from this research carry significant implications for public health and the promotion of a healthy aging process, which involves sustaining functional ability to ensure well-being.
Understanding the extent of noise exposure in various local authorities, particularly in areas where transportation noise exceeds 55 dB on a 24-h basis, is essential.
This study goes one step further to pinpoint areas with a heavier noise burden, allowing for the tailoring of public health interventions in these regions to enhance the quality of life for older residents and support a healthier aging process.
Overall, this research offers a valuable foundation for informed decision-making and targeted strategies to reduce noise-related health risks in affected local authorities, ultimately contributing to the well-being and healthy aging of the population.
Future research should examine the impact of noise pollution on mental health in areas with persistently high depression rates [36] and explore the differences in mental health effects between urban environments characterised by frequent high-intensity sounds, such as police or ambulance sirens, and those with continuous, lower-intensity background noise, such as motorways.
Future research should also explore the spatial relationship between noise pollution and other health outcomes, including hearing loss [37], cardiovascular disease [1, 38], sleep disturbance [28, 39,40,41], cognitive decline [22, 42, 43], metabolic syndrome [44], diabetes [45], obesity [46], dementia [47], and tinnitus [4].







留言 (0)