Higher blood IL-6 levels upon ICU admission were significantly associated with an increased risk of death in non-elderly patients with sepsis. However, no such association was observed in the elderly patients. The significant interaction term between age categories and IL-6 levels further supported these different associations. In contrast, higher blood IL-6 levels were significantly associated with an increased risk of MOD on days 3 and 7 in both non-elderly and elderly patients.
Several studies have shown that higher IL-6 levels are associated with an increased risk of mortality in critically ill patients. A study with a small sample size (n = 142), including adult patients of all ages with sepsis or SIRS (median age [range], sepsis vs. SIRS, 75 [42–98] vs. 68 [37–81] years), suggested that increased serum IL-6 levels were associated with an increased risk of 28-day mortality (HR = 1 pg/mL change, 1.0004) [7]. A study including relatively younger critically ill patients (median age [IQR], 64 [51–74] years) indicated that plasma IL-6 levels > 100.9 pg/mL were associated with worse 90-day mortality (HR 1.91, 95% CI 1.62–2.24) and this association persisted even after adjustment for severity using Simplified Acute Physiology-II score (adjusted HR 1.92, 95% CI 1.63–2.26) [8]. Our results in non-elderly patients demonstrated that higher IL-6 levels were associated with an increased hazard ratio for in-hospital 28-day mortality, which is consistent with these reports.
The elderly patients in our study had significantly higher IL-6 levels at admission than the non-elderly patients. However, there was no significant association between IL-6 levels and risk of mortality in this group. Cytokine expression may differ between elderly and non-elderly individuals under septic conditions. A previous report on human sepsis suggested that patients aged ≥ 70 years showed decreased expression of genes involved in cytokine signaling and innate and adaptive immunity in blood leukocytes compared to patients aged < 50 years [11]. This finding indicates that elderly patients may have a blunted host response, which could contribute to their impaired cytokine expression during sepsis. Meanwhile, animal studies using lipopolysaccharide- or cecal ligation and puncture-induced sepsis showed that blood IL-6 levels were significantly higher in aged mice than in younger mice [24, 25]. This observation suggests that elderly animals may exhibit a more dysregulated host response compared to younger animals, even when subjected to the same insults. Given that the host responses in elderly patients may easily be dysregulated, the blurred cytokine expressions make their dynamics complex and not straightforward. Our study showed similar mortality rates between elderly patients with lower and higher IL-6 levels (Fig. 2). In addition, this outcome may be influenced by altered host responses; elderly patients exhibited high IL-6 levels even among survivors, whereas non-elderly survivors had low IL-6 levels, and non-elderly non-survivors displayed extremely high IL-6 levels (survivors vs. non-survivors: elderly, 1,765 vs. 1,974 pg/mL; non-elderly, 866 vs. 7,932 pg/mL). Age-related changes may influence cytokine dynamics and alter the association between IL-6 levels and mortality.
Unlike its association with mortality, higher blood IL-6 levels were significantly associated with an increased risk of MOD on days 3 and 7 in both the elderly and non-elderly patients. This finding highlights the potential clinical application of IL-6 as a biomarker even in elderly patients. IL-6 has been reported to be associated with organ dysfunction or severity of critical illness. Our previous study showed the blood IL-6 levels in the early phase of ICU admission (days 0, 1, 2) had high predictive values for MOD on days 3 and 7 among seven clinically relevant biomarkers (IL-6, IL-8, IL-10, tumor-necrosis-factor-α, white blood cells, C-reactive protein, and procalcitonin) [6]. A study involving critically ill patients including both with and without sepsis demonstrated that baseline plasma IL-6 levels were associated with the need for future organ support therapies, such as vasopressors/inotropes and renal replacement therapy [8]. In addition, an investigation that included critically ill patients of all ages who visited the emergency department demonstrated that IL-6 was significantly associated with a diagnosis of sepsis based on the sepsis-3 criteria, which is equal to the number of patients with organ dysfunction, with a high diagnostic value (AUC 0.764) [10]. Notably, this study found no significant association between IL-6 levels and 28-day mortality, which is consistent with the results in our elderly patients. Although several studies have reported that higher IL-6 levels are significantly associated with an increased risk of mortality [7, 8], this association remains controversial [26]. Our study demonstrated that higher IL-6 levels significantly increased the risk of MOD but showed no such association with the risk of mortality in elderly patients. Exaggerated inflammation in sepsis directly contributes to early phase deterioration. However, later-phase outcomes such as mortality may be influenced by factors other than inflammation, such as immune senescence. Therefore, the timing of the outcomes may partly explain the different associations in elderly patients. Moreover, non-elderly patients exhibit more robust immune responses and are capable of expressing cytokines more effectively than elderly patients [11], which may contribute to the significant association between IL-6 levels and the risk of mortality observed in non-elderly patients. IL-6 levels may serve as various outcome predictors in non-elderly patients, while it may be a more reliable indicator of the risk of MOD in the early phase rather than the risk of mortality in elderly patients.
Several covariates other than IL-6 levels were significantly associated with the risk of mortality in only one of the groups (non-elderly, number of chronic organ dysfunctions, P = 0.016; elderly, BMI and steroid use prior to sepsis onset, P = 0.027 and 0.002, respectively). Previous studies have suggested that these factors may affect outcomes differently across different age groups. Elderly patients with sepsis or septic shock had higher APACHE II scores than non-elderly patients, while they had similar numbers of chronic organ dysfunctions, suggesting that factors other than chronic organ dysfunction contribute more to severe conditions in elderly patients [27]. Overweight or obese BMI was associated with decreased mortality in patients with sepsis aged > 50, while it was not associated with mortality in those aged ≤ 50 years [20]. Although studies investigating the effects of steroid use before the onset of sepsis are limited, one study that included relatively younger patients with septic shock (median age, 68 years) found that baseline exposure to immunosuppressive therapy was not associated with mortality [28]. Age can be a crucial factor as it influences the association between covariates and outcomes.
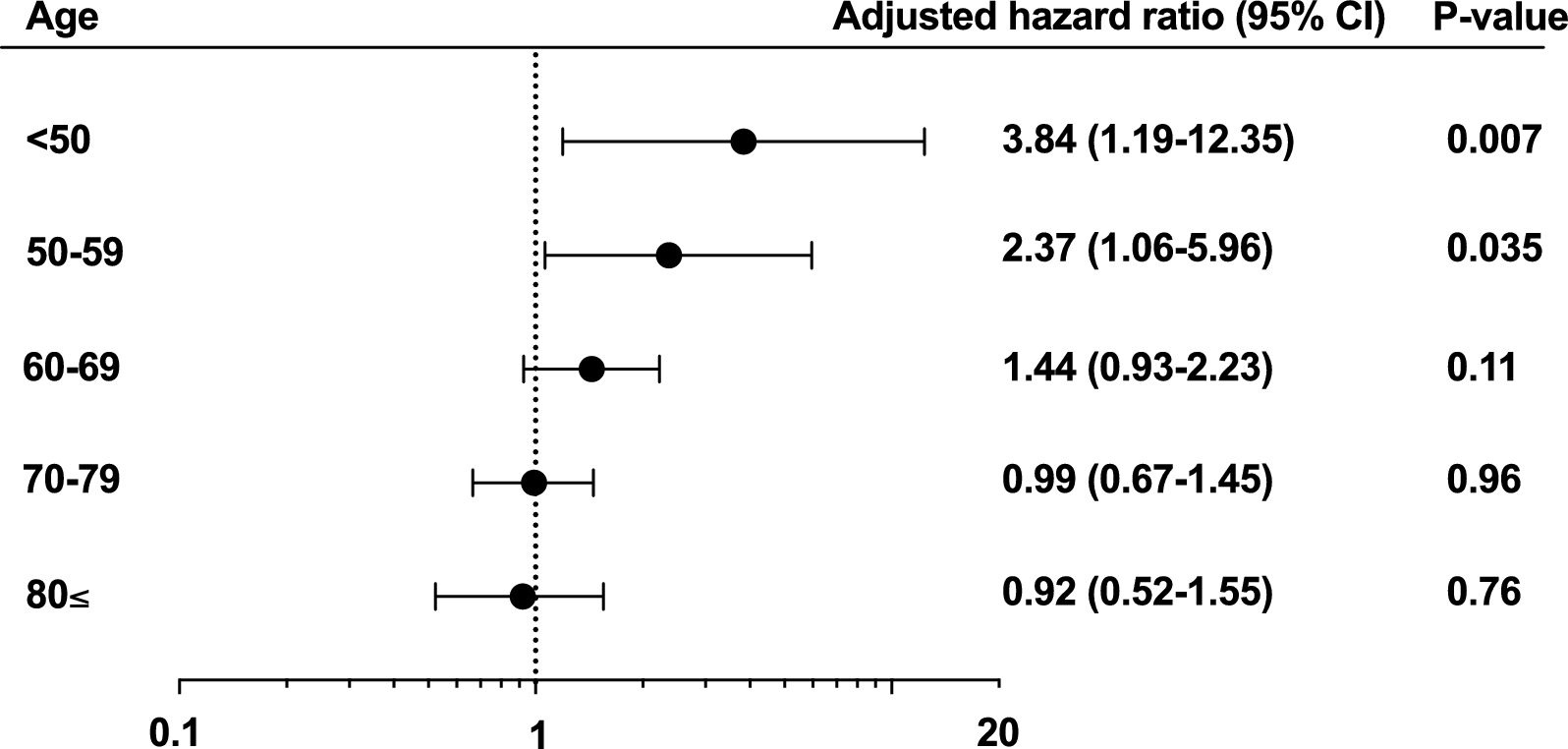
Our study had several limitations. First, this was a single-center retrospective observational study, which may have caused selection, treatment, and misclassification biases. Although information such as comorbidities was retrieved using consistent criteria, some data may still be lacking. Furthermore, while we included more than 500 patients with sepsis, the generalizability of our findings should be investigated. Second, IL-6 levels were not measured based on pre-determined criteria, which may also have introduced selection bias. However, there was no significant difference in the proportion of the patients with missing IL-6 measurements between the non-elderly and elderly groups among those with sepsis (patients with missing IL-6 levels/patients with sepsis: non-elderly vs. elderly, 110/382 [28.8%] vs. 126/373 [33.8%], P = 0.14). Third, we could not determine the precise onset of sepsis, which may affect the timeline of MOD development. The occurrence and clinical course of MOD depend on the timing of the initial insult. Fourth, there is no universally established definition of age in elderly patients. Nonetheless, we conducted a subgroup analysis by dividing the patients into 10-year age groups and found a consistent trend of decreasing association between elevated IL-6 levels and mortality as age increased. This study found associations between IL-6 levels and mortality or MOD across different age groups. Despite these limitations, our findings provide valuable insights into IL-6 levels in patients with sepsis. However, further studies are required to establish a causal link between IL-6 levels and clinical outcomes.





留言 (0)