To our knowledge, this is the first study to report on the burden of headache disorders in Vietnam. The study uses data collected concurrently from the same population as our recently published paper on the prevalence of headache disorders among medical students [6]. Although our study was conducted on a specific population and may not be fully representative of the general population in Vietnam, its findings provide valuable insights that contribute to the growing body of evidence on the burden of headache disorders, both within Vietnam and globally.
The analysis of symptom burden revealed that the average participant-reported headache frequency was 3.6 days per month, consistent with findings from previous studies conducted in Mali (3.5 days/month) [17] and Nepal (3.8 days/month) [18]. However, this frequency was lower compared to studies in Saudi Arabia (4.3 days/month) [14], Cameroon (6.7 days/month) [13], and Mongolia (7.0 days/month) [15]. The mean duration of any headache in our study was 5.3 h, which is shorter than that of studies conduted in Saudi Arabia (8.4 h) [14], Mongolia (11.2 h) [15], and Cameroon (13.0 h) [13]. In the present study, 58% of students with headaches in the past year reported experiencing at least moderate severity, with a mean intensity of 1.6 (mild to moderate on a scale of 1–3), which is similar to that reported in Mongolia (mean intensity of 1.5) [15] but slightly lower than the mean intensities reported in Nepal (2.1) [18], Saudi Arabia (2.3) [14], and Cameroon (2.3) [13]. Additionally, the estimated pTIS indicated that symptoms accounted for an average of 2.8% of the total time among students with headaches. This figure is lower compared to estimates reported in Saudi Arabia (3.6%) [14], Mongolia (9.7%) [15], and Cameroon (9.8%) [13]. The differences observed between this study and previous research may be attributed to several factors. Methodological variations, including differences in sampling techniques, as well as environmental factors such as climate, pollution, and geographical location, could contribute to these disparities [6]. Additionally, sociodemographic variables, including race, age, and sex, along with variations in socioeconomic status, may influence susceptibility across populations [6].
The mean headache-attributed health loss were 1.41% for migraine and 0.06% for tension-type headache (TTH), which is comparable to the estimates reported in Saudi Arabia (1.5% and 0.0%, respectively) [14] and Cameroon (2.05 and 0.1%, respectively) [13]. This can be interpreted as the intermittent symptoms of migraine and TTH being equivalent to a continuous health diminution of 1.41% and 0.06%, respectively. However, these values do not align with the lost productivity adjusted by prevalence estimates for migraine (mean of 4.5 work/school days and 4.1 household days over 3 months) and for TTH (mean of 3.1 work/school days and 2.6 household days over 3 months). This discrepancy has also been observed in several prior studies and may be attributed to several factors, including the potential underestimation of headache-attributed health loss or the influence of additional factors contributing to productivity loss beyond the direct health impact of headaches [13,14,15]. Moreover, premonitory, postdromal, or interictal symptoms, along with headache severity, are not considered in the estimation of lost health, which relies solely on pTIS, a measure that only assesses the duration of headache episodes [14, 19,20,21,22].
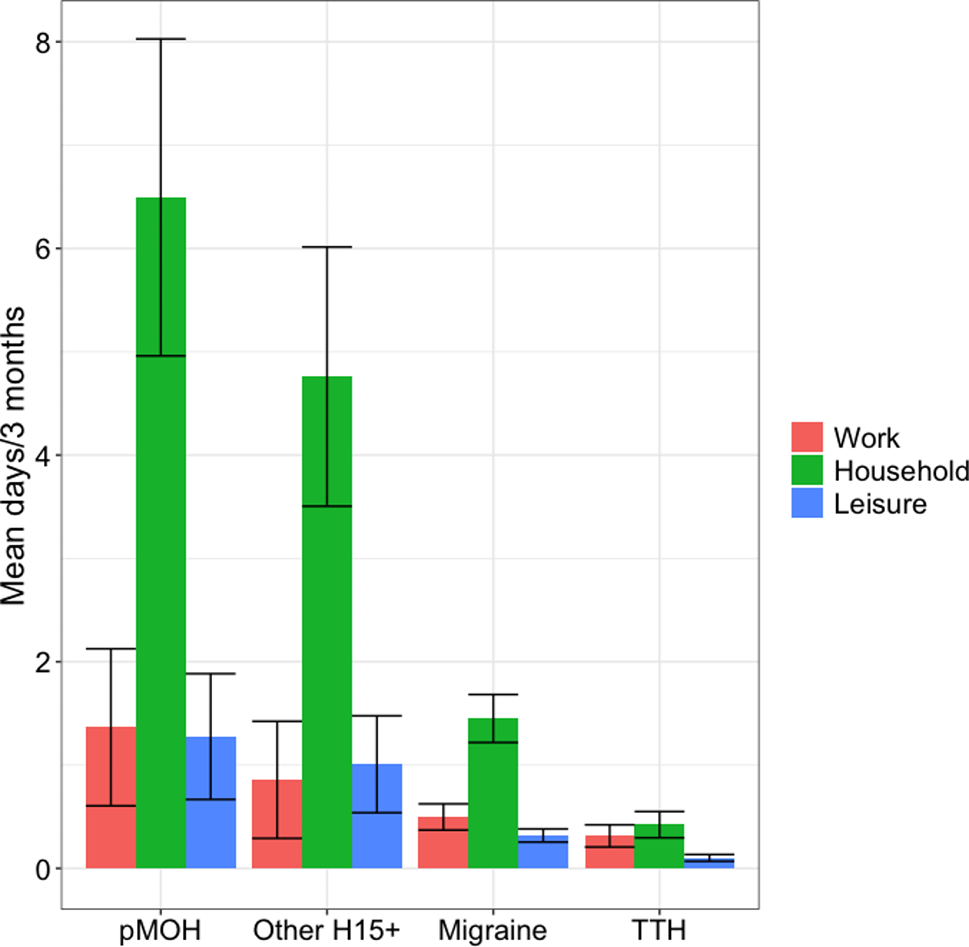
Lost productivity, adjusted for the prevalence in the study population, indicated that, on average, each medical student (with or without headache) lost 3.6 days over a 3-month period from work or school. The estimated productivity loss for household tasks was approximately 3.1 days per 3 months, while withdrawal from social or leisure activities accounted for around 1.4 days per 3 months. These findings are comparable to those reported in studies from Saudi Arabia (2.5, 3.6, and 1.3 days per 3 months, respectively) [14] but higher than those reported in Cameroon (2.5, 2.2, and 0.6 days per 3 months, respectively) [13] and Mongolia (0.8, 1.4, and 0.3 days per 3 months, respectively) [15]. Impairment in household work prevented students from completing essential daily chores, while reduced participation in social or leisure activities left mental and physical needs unmet, potentially contributing to increased stress and other psychological issues. These negative effects, combined with the direct reduction in work or school time due to headache disorders, contribute to a significant decline in productivity among medical students, a group that requires substantial time for study, research, and clinical training. In our study, pMOH and H15 + were more responsible for lost productivity at the individual level compared to migraine and TTH, but they exhibited only a minor impact at the overall population level in the study. This is attributed to their much lower prevalence relative to the other two headache types. Sex differences in days lost between male and female students were minimal in our study, aligning with findings from previous [13,14,15]. Furthermore, these results are consistent with recent trends in Vietnam, where government and community organizations have actively promoted and implemented initiatives to advance sex equality in both work and education.
While HALT data enables a detailed assessment of impaired participation across three domains, it is limited by the absence of an overall participation estimate. A straightforward approach to estimating total impaired participation would involve summing the mean days lost across the three domains (3.6 + 3.1 + 1.4 = 8.1) and dividing by the total number of days in the last three months (8.1/90 = 9.0%); however, this method may lack accuracy [14]. For example, on weekdays (Monday through Friday) with prolonged headache episodes, both work/school and household time may be affected, while on weekends (Saturday or Sunday), headaches may impact household time as well as social/leisure activities. Consequently, participants might count a single day as lost in 2 or even 3 domains. To address this limitation, we incorporated additional impaired participation estimates from HY data (5.5%), yielding a slightly lower result that may reflect an overestimation in the HALT data due to the aforementioned factors. Using both HALT and HY data thus mitigates the individual methodological limitations, providing a more comprehensive understanding of the impaired participation burden of headache disorders within this population [14].
Although the WHOQoL-8 scale was not specifically designed to assess quality of life in patients with headache disorders, it remains valuable for a comprehensive evaluation of symptom burden and impaired participation in this population. In our study, students were diagosed headache were associated with significantly lower QoL compared to students without headaches (WHOQoL-8 mean score: 26.9 vs. 27.7, p < 0.05). In addition, students with other H15 + headache types demonstrated considerably lower average quality of life scores than those with migraine or TTH. These findings, in conjunction with similar results from studies conducted in Mongolia, Cameroon, and Ethiopia, further highlight the significant negative impact of the symptom burden associated with the H15 + group on quality of life [13, 15, 23]. Notably, in our study, the quality of life (QoL) among patients with migraine and tension-type headache (TTH) was nearly identical, with mean WHOQoL-8 summed scores of 27.0 and 27.1, respectively. This finding aligns with results from previous studies conducted in Ethiopia [23], where the mean WHOQoL-8 summed scores for migraine and TTH were 29.5 and 29.3, respectively, and in Cameroon [13], where both headache types had a mean score of 28.0.
Based on established criteria proposed and employed in previous studies to assess health-care needs, nearly half (43.8%) of students in this study were identified as “in need” or likely to “derive substantial benefit” from active headache management and care. These results are slightly higher than those reported in previous studies that applied the same criteria, including those conducted in Saudi Arabia (35.8%) [14], Mongolia (33.2%) [15], and Cameroon (37.0%) [13]. Specifically, in our study, 17.3% of participants met criteria for having headaches on ≥ 15 days per month (pMOH or other) or migraines on ≥ 3 days per month, both conditions indicative of severe symptom burden and widely accepted as thresholds for preventive medication [14, 24]. An additional 26.5% of students met the remaining four criteria (migraine or TTH with pTIS > 3.3% and moderate-to-severe intensity, or migraine/TTH with ≥ 3 days lost from work and/or household duties over the last 3 months), reflecting further health-care needs. Although these latter criteria may seem less stringent than the former, their presence still suggests a meaningful symptom burden with a notable impact on students’ lives, highlighting the necessity for timely, specialized care for this population [14, 15].
Study strengths and limitations
As previously noted, this study’s strengths include its use of a standardized methodology and questionnaire, a adequate sample size, and a high participation rate (94.7%) [6]. Nonetheless, a primary limitation is the inherent reliance of all cross-sectional retrospective studies on participants’ recall, which may introduce recall bias. Furthermore, this study exclusively included medical students, primarily aged 18–24, representing a population with higher educational levels. This demographic specificity limits the generalizability of our findings to the broader population. Additionally, diagnoses were based solely on participants’ self-reported responses, rather than objective measures such as medical records or clinical interviews, which introduces the potential for bias.





留言 (0)