
記住我



This prospective cross-sectional study involved women who attended the postpartum rehabilitation clinic at the First Affiliated Hospital of Gannan Medical University between May 2022 and September 2023. Data collection occurred within 6–8 weeks postpartum. All patients' cesarean section scars were assessed by the same evaluator to ensure consistency in the evaluations. Women with severe organic organ disease, history of prior abdominal surgery, or inability to provide accurate responses were excluded. All patients provided written informed consent. The study was approved by the Ethics Committee of the First Affiliated Hospital of Gannan Medical University (approval number LLSC-2022042802) and was registered in the Chinese Clinical Trial Registry (registration number: ChiCTR2200059785; date of enrollment: 11 May 2022).
ScarAll patients' cesarean section scars were assessed by the same evaluator to ensure consistency in the evaluations. Jinglong and Zhehu pointed out that from a pathological perspective, skin scars are classified into two main categories: normal scars (physiological scars) and abnormal scars (pathological scars). The latter primarily includes hypertrophic scars and keloids. Normal scars are characterized by rapid maturation, no contraction, no increase in width, and collagen formation that is sufficient to maintain strength. They do not protrude above the surface of the tissue and have a normal or near-normal color. If a scar initially appears raised above the skin surface but does not exceed the area of tissue damage, and gradually flattens out over time with symptoms of itching and discomfort subsiding, it is classified as a hypertrophic scar. Conversely, if the scar remains raised above the skin surface, continues to grow, and exceeds the area of tissue damage without flattening on its own—especially if it recurs after simple surgical removal and is larger than the original lesion—this is classified as a keloid [9]. During the data collection process, we did not encounter any patients with keloids. Therefore, we categorized the scars in this study into three types: no scar, normal scar, and hypertrophic scar.
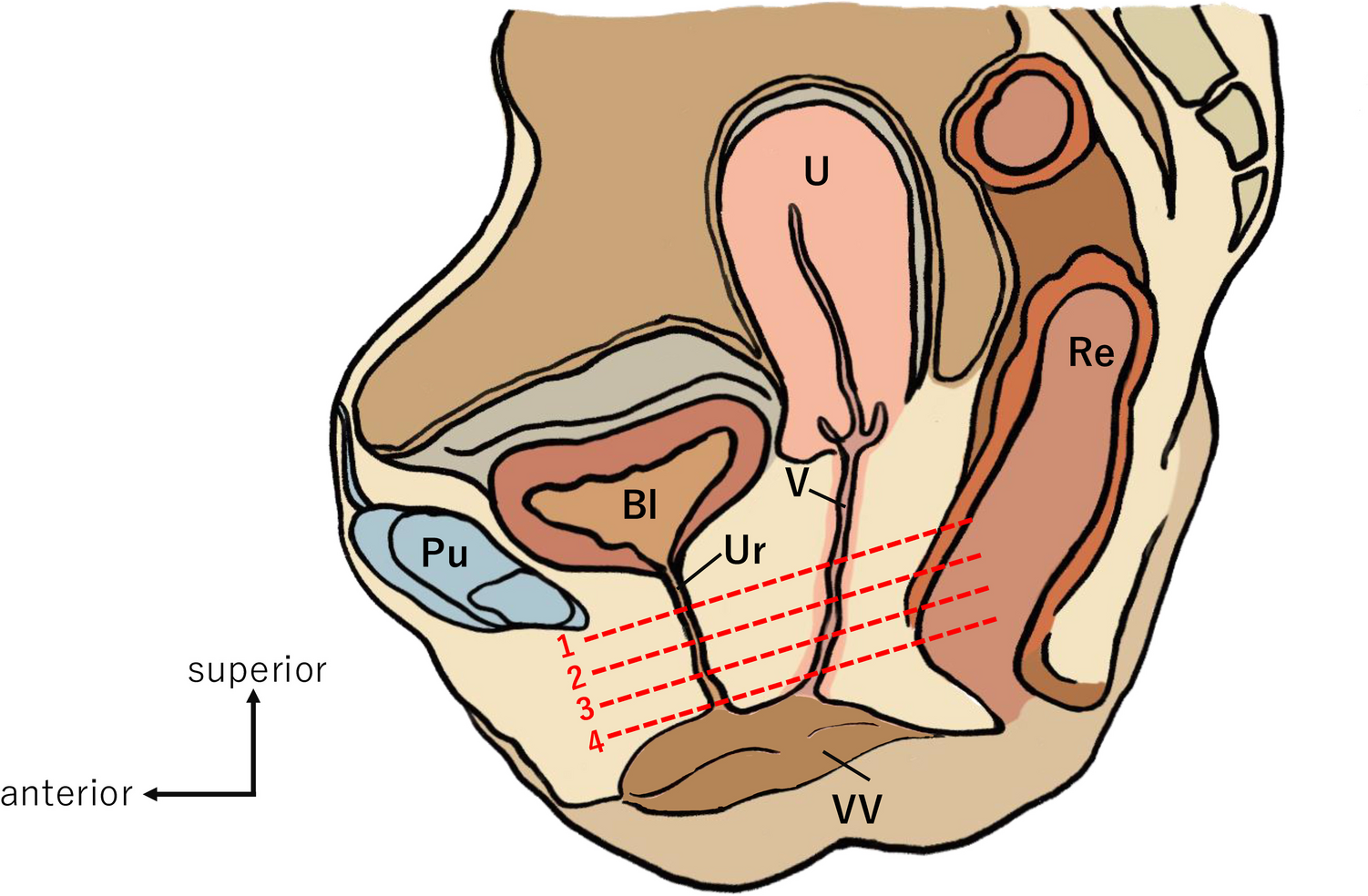
Active Pelvic Floor Muscle ToneWe assessed the active pelvic floor muscle tone and strength in postpartum women using the Glazer protocol. The participants were positioned supine with their upper body at a 120° angle to their lower limbs, and their hips and knees slightly flexed, while maintaining a relaxed overall posture. The vaginal electrode was inserted into the vaginal tube at a depth of 3 to 4 cm, with its metal plate positioned at the 3 to 9 o'clock position. Additionally, a reference electrode was placed on the anterior–superior iliac spine. The participants were instructed by the software to contract and relax their pelvic floor muscles continuously. During pelvic floor muscle contraction, efforts were made to minimize the involvement of the abdominal, gluteal, and thigh adductor muscles.
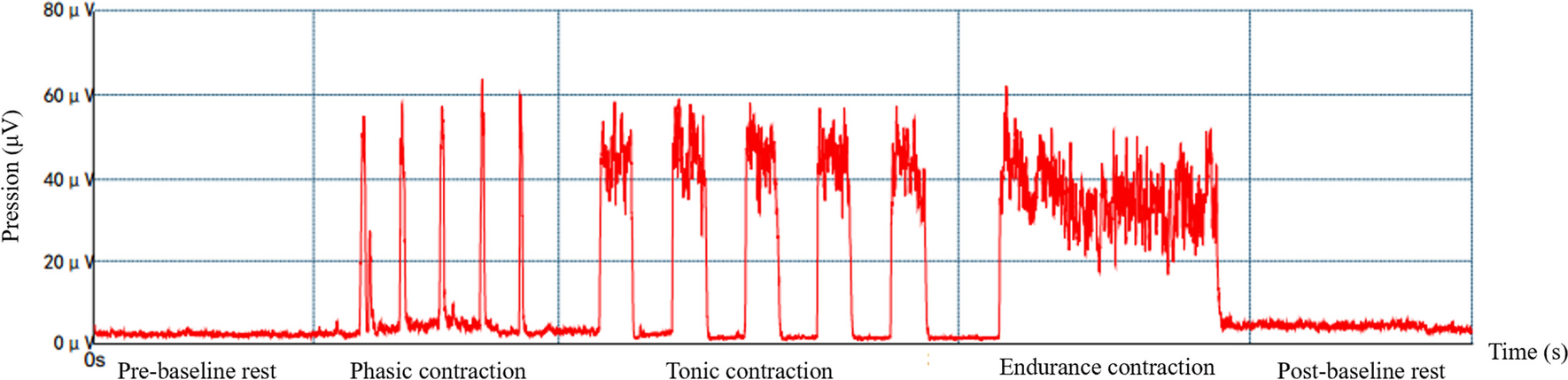
The specific steps are outlined as shown in Fig. 1. During the pre-baseline rest period the active pelvic floor muscle tension is measured under a completely relaxed state for 60 s, including the collection of its average electromyography (EMG) value and variability. The rapid contraction phase assesses the capacity for rapid muscle contraction and recovery. Data collection includes the maximum EMG value, rise time, and fall time. The sustained contraction period consists of continuous muscle contraction for 10 s to collect the average EMG value and variability of sustained muscle contraction. During the endurance contraction stage the endurance of slow muscle contraction is assessed, with the collection of the average EMG value and variability. The post-test resting phase is similar to the pre-test resting state. This phase reflects the pelvic floor muscle active tension in a fully relaxed state for 60 s and involves the collection of its mean EMG value and variability [7, 13]. The Glazer protocol was performed using a pelvic floor muscle sEMG device (MLD A2; Medlander, Nanjing, China).
Fig. 1
Schematic diagram of the Glazer protocol
CovariatesWe included the following variables: age, height, body weight, body mass index (BMI), weight gained during pregnancy, number of pregnancies, primiparous or multiparous, parity, birth weight, gestational age, mode of delivery (vaginal delivery or cesarean section), hypertension [14], type 2 diabetes mellitus (T2DM) [15], thalassemia [16], feeding mode (breast, formula, or mixed feeding), data from intrapelvic sEMG assessment using the Glazer protocol [7]. The selection of these variables is based on their clinical relevance, findings from previous literature, significant covariates identified in univariate regression analysis, and variables for which the change in effect estimates exceeded 10%.
Statistical AnalysisHistogram distribution was employed to assess the normality of the variables. Normally distributed continuous variables were reported as mean ± SD, whereas skewed continuous variables were described as median (interquartile range [IQR]). Categorical variables were presented as frequencies (%). We utilized Chi-squared or Fisher's exact tests for categorical variables, one-way analysis of variance for normally distributed variables, and the Kruskal–Wallis H test for skewed distributions to assess differences among the various scar groups. The Bonferroni correction least significant difference method was applied for multiple comparisons.
The effect of cesarean section scars on active pelvic floor muscle tone was evaluated using linear regression models (regression coefficients β and 95% confidence interval [CI]) with adjustment for major covariables. The selection of these confounders was based on clinical relevance, previous literature, all significant covariates in the univariate analysis, or their associations with the outcomes of interest, or a change in effect estimate exceeding 10%. Potential multicollinearity was assessed using the variance inflation factor (VIF), with an VIF ≥ 5 indicating the presence of multicollinearity. We constructed three models. Model 1 adjusted for age, height, weight, and BMI. Model 2 additionally adjusted for weight gained during pregnancy, number of pregnancies, parity, multiparas, birth weight, and gestational age. Model 3 further adjusted for hypertension, type 2 diabetes, thalassemia, and feeding method.
We employed multiple imputation, based on five replications and a chained equation approach method, to maximize statistical power and minimize bias that may result from missing data [17]. Furthermore, in order to evaluate the robustness of the findings, we conducted a series of sensitivity analyses by combining the normal scar group and the hypertrophic scar group, and then compared them with the no scar group. Within the sensitivity analysis, we applied several additional association inference models, such as propensity score adjustment [18], propensity score matching (PSM) [19], treatment-weighted inverse probability [20], standardized mortality weighting [21], pairwise algorithmic, and overlap weight [22]. All analyses were conducted using the statistical software packages R (http://www.R-project.org, R Foundation) and Free Statistics software version 1.7.1. All statistical tests were two tailed, and statistical significance was defined as p < 0.05.
留言 (0)