
記住我
Crohn’s disease (CD) is a chronic inflammatory gastrointestinal disease characterized by multifactorial pathogenesis and refractoriness. Current therapies focus on reducing intestinal inflammation. As the discovery of novel drug targets and the increasing number of patients with CD refractory to conventional therapies, biologic therapies have gradually come to the forefront. However, with the introduction and clinical availability of infliximab (Knight et al., 1993; van Dullemen et al., 1995), the first tumor necrosis factor α (TNFα) antagonist for the treatment of CD, problems with its efficacy emerged. Among CD patients treated with TNFα antagonists, approximately two-thirds of the patients treated with TNFα antagonists are either primary non-response or loss of response (LOR) over time (Sandborn et al., 2012). Consequently, researchers have developed several new biologic agents based on different immune mechanisms to address the non-response to TNFα antagonists in CD patients: interleukin antagonists like Ustekinumab and Risankizumab (Benson et al., 2011; Singh et al., 2015), anti-integrin monoclonal antibody like Vedolizumab (Soler et al., 2009).
With the popularization of biologics with differing efficacy and safety profiles, clinicians have more therapeutic options when they make medical treatment plans for CD patients. However, they also face tough choices because of the uncertainty of the appropriate positioning of different agents in the disease course. In addition, it is a challenge for clinicians to determine the best pharmacotherapy for a patient who represents a primary non-response or secondary loss of response despite having undergone biologic therapy. These choices involve comprehensive decision-making analysis of the clinical rational medication incorporating patients’ preferences as well as diagnosis and medical recommendations from clinicians. Therefore, researchers collect various clinical data through clinical trials and experiment with different treatment options to achieve clinical rational medication.
Nevertheless, today’s redundant and variable-quality clinical trial results inevitably tire out the clinicians in need, there is a particular demand for systematic reviews to analyze valuable clinical trial results to provide a clear and concise clinical evidence base. Network Meta-Analysis (NMA), a statistical method for comparing multiple treatment options simultaneously through an integrated analysis of both direct and indirect evidence from RCTs, has provided a wealth of evidence on the safety and efficacy of therapies lacking head-to-head RCTs data for many clinical guidelines and Health Technology Assessments (HTAs).
In NMA, Bayesian methods offer several advantages over classical frequentist methods. First, Bayesian methods provide greater flexibility in handling uncertainty by incorporating prior beliefs through prior probability distributions and offering a more comprehensive representation of uncertainty in parameter estimation. Second, Bayesian methods offer advantages in dealing with heterogeneity, allowing for a more nuanced understanding of variability across studies and facilitating the use of complex models, thereby capturing data structure and patterns more effectively (Sutton and Abrams, 2001; Dias et al., 2014a; Higgins and Cochrane, 2019).
With new RCTs being initiated or completed on a daily basis, it is necessary to update the evidence collected, complied and presented by the NMA in order to provide the up-to-date evaluations. In this study, we conducted an updated systematic review and NMA with a Bayesian consistency DerSimonian-Laird random-effects model (Borenstein et al., 2010; Kanters, 2022; Watt and Del Giovane, 2022), using Markov chain Monte Carlo (MCMC) simulation, comparing the relative efficacy and safety of Infliximab, Adalimumab and Certolizumab pegol (three TNFα antagonists), Ustekinumab and Risankizumab (two interleukin antagonists), Vedolizumab (an anti-integrin monoclonal antibody), biosimilars (CT-P13 and BI 695501), and TNFα antagonists combined with immunosuppressants, for adult moderate-to-severe CD patients stratified by history of TNF antagonist treatment in the induction and maintenance therapy. We used Grading of Recommendations Assessment, Development, and Evaluation (GRADE) working group guidance to evaluate the certainty of evidence (Puhan et al., 2014).
2 MethodsThe methods and recommendations of the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) extension statement for NMA for healthcare interventions, and the Cochrane Handbook were used to conduct this systematic review (Hutton et al., 2015; Higgins and Cochrane, 2019). Good research practices from the report of ISPOR (International Society for Pharmacoeconomics and Outcomes Research) for conducting indirect treatment comparisons and NMA for healthcare decision making were referenced (Hoaglin et al., 2011). The study protocol has been prospectively registered in PROSPERO (International Prospective Register of Systematic Reviews, www.crd.york.ac.uk/prospero). The registration number is CRD42023458609.
2.1 Search strategyA comprehensive search of multiple electronic databases, including PubMed, Embase, Web of Science, Scopus, CENTRAL (Cochrane Central Register of Controlled Trials), ClinicalTrials.gov and ICTRP (International Clinical Trials Registry Platform), from inception to 8 June 2023, without language or geographic area restrictions were conducted. MeSH/Emtree words combined with free words were used for the literature search (see Supplementary Table S1 in the Supplementary File 1 [SF1], full search strategy).
2.2 Selection criteriaTwo investigators independently searched the study titles, abstracts and full texts of relevant studies, to identify articles of interest based on the following inclusion and exclusion criteria.
The selection criteria were in strict accordance with the PICOS (Patients, Intervention, Comparators, Outcomes, Study designs) principle. Study included in this NMA were phase Ⅱ or Ⅲ RCTs meeting the following criteria: (1) including adult (18–75 years of age) patients with moderate-to-severe CD (defined by CDAI 220–450); (2) receiving a biologic treatment with TNFα antagonists (Infliximab, Adalimumab or Certolizumab pegol), anti-interleukin (Ustekinumab, Risankizumab), anti-integrin (Vedolizumab), either alone or in combination with immunosuppressants, and their biosimilars, as the first-line biologic or after previous biologic exposure; (3) minimum duration of therapy of 4 weeks for trials reporting induction of response or remission in active disease and 22 weeks in trials reporting maintenance of response or remission; (4) compared to placebo or another medication for CD patients; (5) reporting induction of clinical remission (defined by a CDAI <150) or clinical response (defined by a reduction in the CDAI ≥70 points compared to baseline [CDAI-70], some studies defined the clinical response threshold of CDAI as 100 [CDAI-100], while some reported both CDAI-100 and CDAI-70), maintenance of remission or clinical response (among patients with clinical response to induction therapy in re-randomization trials and among all patients in treat-through trials), or safety (adverse events [AEs], serious adverse events [SAEs], and serious infections [SIs] as defined by the study authors). Only trials conducted in biologic and immunosuppressant naïve patients, in which patients were initiated on biologic monotherapy alone and compared with biologics and immunosuppressants in combination, were included as trials of combination therapy. In contrast, trials specifically enrolling immunosuppressant failed patients to evaluate a single biologic therapy or to compare two or more biologic therapies were included as trials of respective biologic monotherapy.
We excluded studies where: (1) trials of biologics to prevent postoperative recurrence; (2) trials comparing biologic treatment with surgical treatment; (3) pilot studies; (4) trials comparing therapeutic drug monitoring (TDM) with standard therapy; (5) trials with treatment failure or occurrence of complications as the primary end point; (6) trials of the effect of differences in baseline characteristics (C-reactive protein, prior anti-TNFα therapy, severity and disease distribution) on efficacy; (7) trials with unspecified interventions (a class but not a precise medication was specifical); (8) trials of the withdrawal of medications; (9) trials comparing the optimized dosing regimen by pharmacokinetic dashboard (combined with TDM in the OPTIMIZE [Proactive infliximab optimization using a pharmacokinetic dashboard versus standard of care in patients with Crohn’s disease] trial) with the standard dosing regimen; (10) trials of the effect of different preoperative medications on postoperative complications; (11) trials of dosing interval lengthening in maintenance phase; (12) early terminated trials; (13) trials without results; (14) trials included patients with other subtypes of inflammatory bowel diseases (IBD, CD is a subtypes of IBD); (15) reviews, letters, conference abstracts, animal studies; (16) trials of novel therapies without reported phase Ⅲ data; (17) trials of advanced therapies not frequently used for the treatment of moderate-to-severe CD in clinical practice.
2.3 Data analysisTwo study investigators (Haohang Su and Shengwei Xiao) independently rated the risk of bias of included RCTs using RoB 2 (version 2 of the Cochrane risk-of-bias tool for randomized trials) (Sterne et al., 2019). Any discrepancies were resolved by consensus or in consultation with a third reviewer (Xixiao Yang). Five domains (randomization process, deviations from intended interventions, Missing outcome data, measurement of the outcome, selection of the reported result) were assessed separately as “low risk”, “high risk”, or “some concerns” and analyzed together to produce a final risk of bias judgement for each study (see Supplementary Figure S1 in SF1, traffic light plot of the risk of bias assessment). A sensitivity analysis was conducted excluding the inferior quality trials.
A standardized data extraction form was used to capture study-, participant-, disease-, and treatment-related characteristics, and was done independently by two investigators. Any discrepancies were resolved by consensus or in consultation with the third reviewer. The most complete report of trial data, based on intent-to-treat analysis principles for efficacy outcomes and last observation carried forward for safety outcomes, was used for extraction if study results were reported in multiple publications. In addition, Individual patient-level data was not sought in this review.
The primary efficacy outcome chosen in induction trials included achievement of clinical response (defined by a reduction in the CDAI ≥70 [CDAI-70] or ≥100 [CDAI-100] points compared to baseline). Secondary outcome was achievement of clinical remission, defined by a CDAI <150. For maintenance trials, the primary efficacy outcome was maintenance of clinical remission, secondary outcomes were CDAI-70 and CDAI-100. The results of evaluations of CDAI-100 as the predominant for interpretation when discrepancies between the results of CDAI-70 and CDAI-100 in the evaluations of clinical response occurred (Sands et al., 2024). Both responder re-randomization and treat-through trials were included, although data informing remission rates among induction responders was preferentially used when available for the primary maintenance outcome in treat-through studies. A sensitivity analysis was conducted excluding treat-through trials. The safety outcomes evaluated in induction or maintenance trials were adverse events (AEs), serious adverse events (SAEs), and serious infections (SIs), as defined by the primary study authors (included the timepoint for the safety summary).
Data from a medication’s approved dosage and administration was used, but the included subcutaneous injections formulation of Vedolizumab (Vedolizumab SC) evaluated in the VISIBLE-2 trial is an exception because of its potential clinical advantage. In trials had multiple outcomes from different times, we extracted the data from week 6 for the induction phase (if data from week 6 were not available, the earliest data from week 4 onwards were extracted), and the latest result for the maintenance phase. Long-term open-label trials were not used. The denominator used in all trials was based on intent-to-treat analysis with dropouts or missing data treated as non-responders for remission and response outcomes; last-observation-carried-forward (LOCF) or observed-case (OC) was used for missing continuous values; missing categorical variables were imputed using non-responder imputation (NRI).
Other extracted covariables included location of trial conduct, number of trials centers or sites, sample size (included the number of TNF antagonist-naïve patients and total sample size), trial design (received medication, dosage regimen, duration of intervention, and randomization), dosage and schedule of active/comparator group, severity of CD at randomization, definition of outcomes, outcome timepoints, concomitant medications (divided into active group and placebo/comparator group, medications included aminosalicylates, immunosuppressants, and corticosteroids).
A Bayesian random-effects model was built given the anticipated differences between trials with respect to patient enrolment criteria, patient populations, outcome timepoint of evaluations and interventions (assessments of model fit are presented in the results). A sensitivity analysis was conducted changing the original random-effects model to a Mantel-Haenszel fixed-effect model. Pooled odds ratios (ORs) with 95% credible interval (CrI) were estimated, and statistical heterogeneity was evaluated using the I2 statistic. We also conducted a sensitivity analysis using relative risk (RR) as the effect size.
In the Bayesian model for evaluating the induction and maintenance of clinical remission in moderate-to-severe CD patients, the MCMC parameters were set to 4 chains, 20,000 adaptation iterations, 200,000 total iterations, burn-in iterations were half of total iterations rounded down and the thin parameter was 1. The priors on the baseline and relative treatment effects were defined as independent normal priors (used with mean 0 and standard deviation 15u, where u is the largest maximum likelihood estimator in single trials), an uniform distribution with range 0 to u was used as the prior on variance of relative treatment effects (van Valkenhoef et al., 2012). In the other evaluations, the total iterations were set to 50,000. A sensitivity analysis was conducted changing the original standard deviation of independent normal priors of the baseline treatment effects and relative treatment effects to 10u.
Statistical heterogeneity of these various outcomes was demonstrated by forest plots (see Supplementary Figures S2A–2E; Supplementary Figures S3–S7 in SF1, network plots and forest plots of direct comparisons). Small study effects and publication bias were examined by assessing for funnel plot asymmetry (see Supplementary Figures S8–S14 in SF1, all funnel plots). A sensitivity analysis was conducted excluding the trials which data points fell outside the 90% confidence interval in the funnel plots. Model fit was assessed by computing the Deviance Information Criteria (DIC) and producing a leverage plot, all leverage plots are presented in Supplementary Figures S15–S19 (Dias et al., 2014a). MCMC model convergence was assessed by Brooks-Gelman-Rubin diagnosis plot, computing shrink factor and potential scale reduction factor (PSRF), all assessment results of convergence are presented in Supplementary Figures S20–S24 in SF1. The relative ranking of agents for each outcome was expressed using rankogram (a kind of bar chart showing the probability of each treatment ranking in each rank) and the surface under the cumulative ranking curve (SUCRA). Higher SUCRA values correspond to better efficacy or safety outcomes for induction/maintenance (better means that the corresponding intervention is more effective or has lower safety risks). The relative effectiveness of biologics for each outcome was compared in league heat plot and forest plot. All plots of comparative evaluation results are presented in Supplementary Figures S25–S39 in SF1.
In inconsistency analysis, we plotted the posterior mean deviance contributions of the individual data points for the consistency model and the inconsistency model along with the line of equality (see Supplementary Figure S40 in SF1, all consistency vs. inconsistency plots) and analyzed the anomalous data points specifically (Dias et al., 2014b). Finally, we used GRADE working group guidance to evaluate the certainty of evidence (Puhan et al., 2014) (see Supplementary Tables S2–S6 in SF1). All data analysis described above were conducted using ‘BUGSnet’ package in R statistical software (version 4.3.1). (Beliveau et al., 2019).
3 Results3.1 Search resultsThe search strategy yielded 16,252 citations, of which 3,214 were duplicates and removed. Of the remaining 13,038 records that were screened, 103 full text articles were reviewed 31 trials in 28 studies were eligible for inclusion (see Supplementary Figure S41 in SF1, flow diagram of selection). A total of 22 RCTs were involved in evaluations of induction efficacy and safety in patients with moderate-to-severe CD, of which 13 and 8 RCTs evaluated induction efficacy in TNF antagonist-naïve and -experienced patients, respectively. There were 20 RCTs evaluating maintenance efficacy and safety in patients with moderate-to-severe CD, including 11 and 6 RCTs evaluating maintenance efficacy in TNF antagonist-naïve and experienced patients, respectively.
Patient and trial-level characteristics for induction and maintenance are summarized in Supplementary Tables S7–S8 in SF1, five of the included trials were completed in a single country, and the rest were completed in multiple centers or sites. Patient inclusion and exclusion criteria varied among these trials, mainly manifested in severity of CD (3 RCTs were defined as CDAI 220–400, the DIAMOND trial was defined as CDAI ≥220 (Matsumoto et al., 2016), all others were defined as CDAI 220–450), TNF antagonists using history (8 RCTs excluded TNF antagonist-experienced patients and 15 RCTs included patients with prior failure of TNF antagonists, the other trials required conventional therapy failure as an inclusion criterion), and concomitant medications. On the comparator settings, one head-to-head, active-comparator trial (SEAVUE) comparing Ustekinumab with Adalimumab was identified (Sands et al., 2022); two head-to-head, active-comparator trials (the SONIC, DIAMOND trials) comparing biologic with combination therapy (biologic combined with azathioprine) were identified (Colombel et al., 2010; Matsumoto et al., 2016); and two three-arm trials (the ACCENT-1 and FORTIFY trials) comparing different doses of Infliximab or Risankizumab were identified (Hanauer et al., 2002; Ferrante et al., 2022). One placebo-controlled trial evaluating Vedolizumab SC was included, although subcutaneous injections formulation has not been approved (by U.S. Food and Drug Administration [FDA]) as an administration of Vedolizumab in the treatment of CD. Two head-to-head, biosimilar-comparator trials (Infliximab and Adalimumab were each compared with their biosimilars [CT-P13 and BI 695501]) were identified (Ye et al., 2019; Hanauer et al., 2021). All of the included trials were re-randomization trials, except for the SONIC, DIAMOND, SEAVUE, PRECISE-1 trials, which were treat-through trials. All induction or maintenance outcomes were uniformly evaluated based on standard definition of the CDAI, between weeks 4 and 10 for induction therapy phase and weeks 22 and 60 for maintenance phase, and the results of secondary outcomes are presented in Supplementary Result 1-4 in SF1.
3.2 Efficacy in overall patients with Crohn’s disease3.2.1 Induction therapyA total of 22 RCTs including 6,427 moderate-to-severe CD patients evaluated induction clinical response (CDAI-70 and CDAI-100) after treatment with Infliximab (n = 3 trials, one biosimilar-comparator trial [CT-P13] and one combination-therapy-comparator trial [combined with azathioprine] were included) (Targan et al., 1997; Colombel et al., 2010; Ye et al., 2019), Adalimumab (n = 6 trials, one biosimilar-comparator trial [BI 695501] and one combination-therapy-comparator trial [combined with azathioprine] were included) (Hanauer et al., 2006; Sandborn et al., 2007c; Watanabe et al., 2012; Matsumoto et al., 2016; Chen et al., 2020; Hanauer et al., 2021), Certolizumab Pegol (n = 2 trials) (Sandborn et al., 2007a; Sandborn et al., 2011), Ustekinumab (n = 4 trials, included one active-comparator [Adalimumab] trial) (Sandborn et al., 2012; Feagan et al., 2016; Sands et al., 2022), Risankizumab (n = 3 trials) (Feagan et al., 2017; D'Haens et al., 2022), Vedolizumab (n = 4 trials) (Sandborn et al., 2013; Sands et al., 2014; Takeda, 2017; Watanabe et al., 2020).
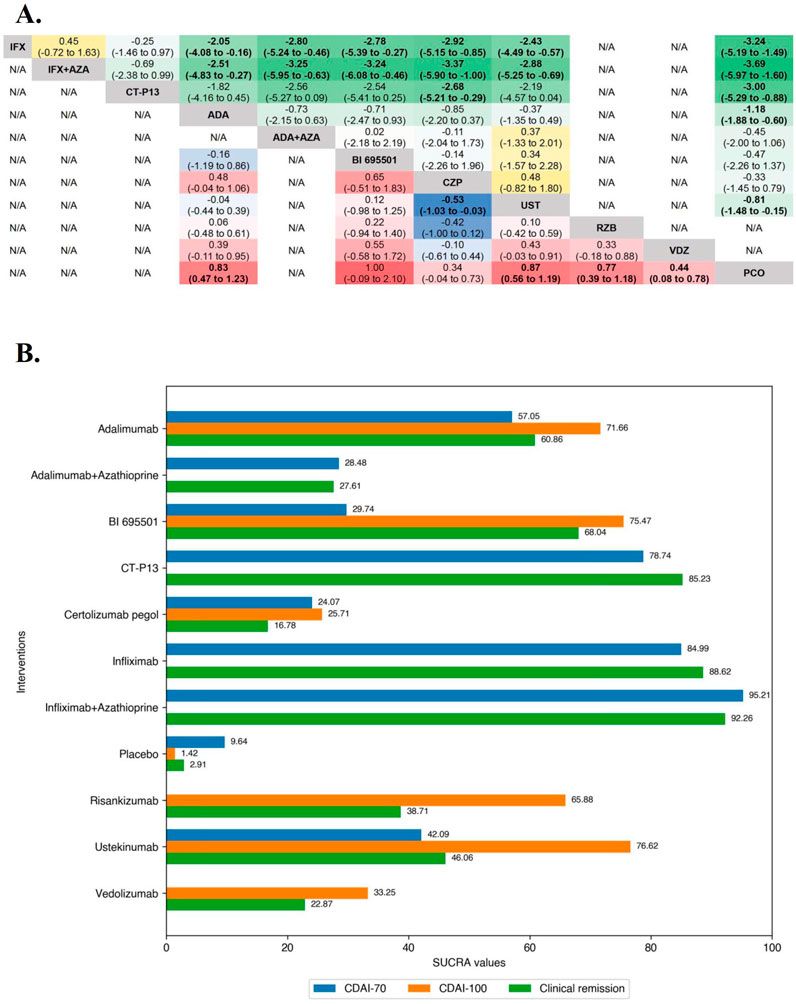
In the evaluation of inducing CDAI-70 in moderate-to-severe CD patients, funnel plots did not show evidence of publication bias or small study effects after including outcome timepoint as a moderator, and also suggests that this part of the heterogeneity caused by differences in outcome timepoint contributed to the asymmetry of the funnel plot. The Brooks-Gelman-Rubin diagnosis plot and the calculated PSRF indicated convergence of the MCMC sampling. On direct meta-analysis, all agents except Risankizumab and Vedolizumab, which CDAI-70 were not evaluated in included RCTs, were significantly superior to placebo for inducing CDAI-70. Neither Infliximab nor Adalimumab had significant superiority over their respective biosimilars or combinations with azathioprine. On network meta-analysis, Infliximab alone and Infliximab in combination with azathioprine were both significantly superior to Adalimumab, Ustekinumab, BI 695501, Adalimumab and azathioprine in combination, and Certolizumab Pegol. The evidence also supported a significant superiority of CT-P13 over Certolizumab Pegol (log OR 2.68 [95% CrI: 0.29, 5.21], Figure 1A). Overall, Infliximab in combination with azathioprine (SUCRA 95.21) and Infliximab alone (SUCRA 84.99) were ranked highest (Figure 1B).

Figure 1. (A) SUCRA (the surface under cumulative ranking curve) values of each intervention in efficacy evaluations of induction therapy in overall patients with moderate-to-severe Crohn’s disease. SUCRA values are expressed on a scale from 0 to 100. The closer the value is to 100, the more likely the intervention is to be among the most effective. Conversely, the closer the value is to 0, the less effective the treatment is likely to be. (B) League heat plot of mixed comparisons of inducing clinical response (defined by a reduction in the CDAI [Crohn’s Disease Activity Index] ≥70 [CDAI-70] or ≥100 [CDAI-100] points compared to baseline) between included biologic agents in overall patients with moderate-to-severe Crohn’s disease, reporting odds ratios on the logarithmic scale (log OR) with 95% confidence intervals. Log OR greater or less than 0 are indicated in red/yellow or blue/green, respectively, in comparisons of inducing CDAI-100/CDAI-70, and the darker the color, the greater the odds ratios. Bold type represents statistically significant superiority/inferiority of the intervention over the comparator.
In the evaluation of inducing CDAI-100 in moderate-to-severe CD patients, the results of funnel plot and model convergence assessments were within appropriate and controllable range. The leverage plot suggested that the SEAVUE trial may have contributed to the poor model fit and a sensitivity analysis was conducted excluding the SEAVUE trial. On direct meta-analysis, all agents except Infliximab (CDAI-100 were not evaluated in included RCTs) and Vedolizumab (OR 1.49 [95% CI: 0.94, 2.37]), were significantly superior to placebo for inducing CDAI-100. There was no benefit of Adalimumab over BI 695501 (OR 0.86 [95% CI: 0.35, 2.15]) for inducing CDAI-100, and similarly no benefit of Ustekinumab over Adalimumab (OR 1.09 [95% CI: 0.71, 1.67]). On network meta-analysis, Ustekinumab was significantly superior to Certolizumab Pegol (log OR 0.53 [95% CrI: 0.03, 1.03], Figure 1A). Ustekinumab (SUCRA 76.62), BI 695501 (SUCRA 75.47), and Adalimumab (SUCRA 71.66) were ranked highest (Figure 2B).

Figure 2. (A) SUCRA (the surface under cumulative ranking curve) values of each intervention in efficacy evaluation of maintenance therapy in overall patients with moderate-to-severe Crohn’s disease. SUCRA values are expressed on a scale from 0 to 100. The closer the value is to 100, the more likely the intervention is to be among the most effective. Conversely, the closer the value is to 0, the less effective the treatment is likely to be. (B) League heat plots of mixed comparisons of maintaining clinical remission (defined by a CDAI [Crohn’s Disease Activity Index] < 150) between included biologic agents in overall patients with moderate-to-severe Crohn’s disease, reporting odds ratios on the logarithmic scale (log OR) with 95% confidence intervals. Log OR greater or less than 0 are indicated in red or blue, respectively, in comparisons of maintaining clinical remission, and the darker the color, the greater the odds ratios. Bold type represents statistically significant superiority/inferiority of the intervention over the comparator.
3.2.2 Maintenance therapyOverall, 20 RCTs including 4,834 patients with moderate-to-severe CD evaluated maintenance clinical remission. Therapies that were evaluated included Infliximab (n = 4 trials, included one biosimilar-, one combination-therapy-comparator trial and one three-arm trial [the ACCENT-1 trial]) (Rutgeerts et al., 1999; Hanauer et al., 2002; Colombel et al., 2010; Ye et al., 2019), Adalimumab (n = 6 trials, included one biosimilar-comparator trial and one combination-therapy-comparator trial) (Colombel et al., 2007; Sandborn et al., 2007b; Rutgeerts et al., 2012; Watanabe et al., 2012; Matsumoto et al., 2016; Hanauer et al., 2021), Certolizumab Pegol (n = 2 trials) (Sandborn et al., 2007a; Schreiber et al., 2007), Ustekinumab (n = 3 trials, one active-comparator [Adalimumab] trial was included) (Sandborn et al., 2012; Feagan et al., 2016; Ferrante et al., 2022; Sands et al., 2022), Risankizumab (n = 1 trial, one three-arm trial [the FORTIFY trial]) (Ferrante et al., 2022), Vedolizumab (n = 4 trials, included one trial evaluating Vedolizumab SC) (Sandborn et al., 2013; Takeda, 2017; Watanabe et al., 2020; Vermeire et al., 2022).
In the evaluation of maintaining clinical remission in moderate-to-severe CD patients, funnel plots did not show evidence of publication bias or small study effects, the Brooks-Gelman-Rubin diagnosis plot and the calculated PSRF indicated convergence of the MCMC sampling. On direct meta-analysis, all agents included Vedolizumab SC (OR 1.77 [95% CI: 1.15, 2.71]) were significantly superior to placebo. Comparisons between treatment groups of biologic agents (5 mg/kg maintenance regimen of Infliximab [IFX-5] vs. 10 mg/kg maintenance regimen of Infliximab [IFX-10] in the ACCENT-1 trial and 180 mg maintenance regimen of Risankizumab [RZB-180] vs. 360 mg maintenance regimen of Risankizumab [RZB-360] in the FORTIFY trial) were not statistically different in either of the two included three-arm trials. Neither the corresponding biosimilar nor combination of azathioprine had a significant effect on the efficacy of infliximab or adalimumab compared with monotherapy. There was no benefit of Ustekinumab over Adalimumab (OR 1.18 [95% CI: 0.78, 1.79]). On network meta-analysis, Adalimumab (SUCRA 81.05), IFX-10 (SUCRA 76.60), Infliximab in combination with azathioprine (SUCRA 72.81), Adalimumab in combination with azathioprine (SUCRA 64.98) were ranked highest (Figure 2).
3.3 Efficacy in TNF antagonist-naïve patients with Crohn’s disease3.3.1 Induction therapyA total of 14 induction RCTs including 3,050 TNF antagonist-naïve patients with moderate-to-severe CD evaluated induction clinical response (CDAI-70 and CDAI-70) after treatment with Infliximab (n = 3 trials, included one biosimilar-, one combination-therapy-comparator trial) (Targan et al., 1997; Colombel et al., 2010; Ye et al., 2019), Adalimumab (n = 4 trials, included one combination-therapy-comparator trial) (Hanauer et al., 2006; Watanabe et al., 2012; Matsumoto et al., 2016; Chen et al., 2020), Certolizumab Pegol (n = 2 trials) (Sandborn et al., 2007a; Sandborn et al., 2011), Ustekinumab (n = 2 trials, included one active-comparator [Adalimumab] trial) (Feagan et al., 2016; Sands et al., 2022), Vedolizumab (n = 3 trials) (Sandborn et al., 2013; Sands et al., 2014; Watanabe et al., 2020).
In the evaluation of inducing CDAI-70 in TNF antagonist-naïve CD patients, the results of funnel plot, model fit and convergence assessments do not require any special attention. On direct meta-analysis, Infliximab (OR 22.00 [95% CI: 5.17, 93.56]) and Adalimumab (OR 4.46 [95% CI: 2.08, 9.56]) were significantly superior to placebo, and the other biologic agents were not evaluated for CDAI-70 in the included RCTs. Similarly, for both Infliximab (OR 0.64 [95% CI: 0.40, 1.02]) and Adalimumab (OR 2.05 [95% CI: 0.83, 5.08]), there was no benefit of their monotherapies over combinations with azathioprine, and Infliximab did not differ significantly from CT-P13 (OR 1.28 [95% CI: 0.71, 2.30]) for inducing CDAI-70. On network meta-analysis, Infliximab in combination with azathioprine (SUCRA 82.68) and Infliximab alone (SUCRA 72.54) were ranked highest (Figure 3).

Figure 3. (A) SUCRA (the surface under cumulative ranking curve) values of each intervention in efficacy evaluations of induction therapy in tumor necrosis factor antagonist-naïve patients with moderate-to-severe Crohn’s disease. SUCRA values are expressed on a scale from 0 to 100. The closer the value is to 100, the more likely the intervention is to be among the most effective. Conversely, the closer the value is to 0, the less effective the treatment is likely to be. (B) League heat plots of mixed comparisons of inducing clinical response (defined by a reduction in the CDAI [Crohn’s Disease Activity Index] ≥70 [CDAI-70] or ≥100 [CDAI-100] points compared to baseline) between included biologic agents in tumor necrosis factor antagonist-naïve patients with moderate-to-severe Crohn’s disease, reporting odds ratios on the logarithmic scale (log OR) with 95% confidence intervals. Log OR greater or less than 0 are indicated in red/yellow or blue/green, respectively, in comparisons of inducing CDAI-100/CDAI-70, and the darker the color, the greater the odds ratios. Bold type represents statistically significant superiority/inferiority of the intervention over the comparator.
In the evaluation of inducing CDAI-100 in TNF antagonist-naïve CD patients, all but Infliximab, which CDAI-100 was not evaluated in included RCTs, were significantly superior to placebo on direct meta-analysis, and there was no benefit of Ustekinumab over Adalimumab (OR 1.09 [95% CI: 0.71, 1.67]). On network meta-analysis, Ustekinumab (SUCRA 84.50) and Adalimumab (SUCRA 82.08) were ranked highest (Figure 3).
3.3.2 Maintenance therapyOnly maintenance clinical remission was evaluated for TNF antagonist-naïve/experienced patients due to the lack of clinical data on the maintenance CDAI-70 and CDAI-100 to form a network. Overall, 11 RCTs including 2,335 TNF antagonist-naïve patients with moderate-to-severe CD evaluated maintenance clinical remission. Therapies that were evaluated included Infliximab (n = 4 trials, included one biosimilar-comparator trial, one combination-therapy-comparator trial and on three-arm trial [the ACCENT-1 trial]) (Rutgeerts et al., 1999; Hanauer et al., 2002; Colombel et al., 2010; Ye et al., 2019), Adalimumab (n = 2 trials, included one combination-therapy-comparator trial) (Colombel et al., 2007; Matsumoto et al., 2016), Ustekinumab (n = 2 trials, included one active-comparator trial) (Feagan et al., 2016; Sands et al., 2022), Vedolizumab (n = 3 trials, included one trial evaluating Vedolizumab SC) (Sandborn et al., 2013; Watanabe et al., 2020; Vermeire et al., 2022).
In the evaluation of maintaining clinical remission in TNF antagonist-naïve patients, the results of funnel plot, model fit and convergence assessments do not require any special attention. On direct meta-analysis, all but Ustekinumab (OR 1.96 [95% CI: 0.89, 4.34]) and Vedolizumab SC (OR 1.26 [95% CI: 0.67, 2.36]) were significantly superior to placebo, and comparisons between active agent regimens did not show significant differences. On network meta-analysis, IFX-10 (SUCRA 68.98), Infliximab in combination with azathioprine (SUCRA 67.01), and Adalimumab alone (SUCRA 66.56) were ranked highest (Figures 4A, B).

Figure 4. (A) SUCRA (the surface under cumulative ranking curve) values of each intervention in evaluation of maintaining clinical remission in tumor necrosis factor antagonist-naïve/experienced patients with moderate-to-severe Crohn’s disease. SUCRA values are expressed on a scale from 0 to 100. The closer the value is to 100, the more likely the intervention is to be among the most effective. Conversely, the closer the value is to 0, the less effective the treatment is likely to be. (B) League heat plots of mixed comparisons of maintaining clinical remission (defined by a CDAI [Crohn’s Disease Activity Index] < 150) between included biologic agents in tumor necrosis factor antagonist-naive patients with moderate-to-severe Crohn’s disease, reporting odds ratios on the logarithmic scale (log OR) with 95% confidence intervals. Log OR greater or less than 0 are indicated in red or blue, respectively, in comparisons of maintaining clinical remission, and the darker the color, the greater the odds ratios. Bold type represents statistically significant superiority/inferiority of the intervention over the comparator. (C) League heat plots of mixed comparisons of maintaining clinical remission (defined by a CDAI [Crohn’s Disease Activity Index] < 150) between included biologic agents in tumor necrosis factor antagonist-experienced patients with moderate-to-severe Crohn’s disease, reporting odds ratios on the logarithmic scale (log OR) with 95% confidence intervals. Log OR greater or less than 0 are indicated in red or blue, respectively, in comparisons of maintaining clinical remission, and the darker the color, the greater the odds ratios. Bold type represents statistically significant superiority/inferiority of the intervention over the comparator.
3.4 Efficacy in TNF antagonist-experienced patients with Crohn’s disease3.4.1 Induction therapyOverall, 10 RCTs including 2,131 TNF antagonist-experienced patients with moderate-to-severe CD evaluated induction clinical response (CDAI-70 and CDAI-70). Therapies that were evaluated included Adalimumab (n = 2 trials) (Sandborn et al., 2007c; Watanabe et al., 2012), Certolizumab Pegol (n = 1 trial) (Sandborn et al., 2007a), Ustekinumab (n = 3 trials) (Sandborn et al., 2012; Feagan et al., 2016), Risankizumab (n = 1 trial) (Feagan et al., 2017), and Vedolizumab (n = 3 trials) (Sandborn et al., 2013; Sands et al., 2014; Watanabe et al., 2020).
In the evaluation of inducing CDAI-70 in TNF antagonist-experienced CD patients, the results of funnel plot, model fit and convergence assessments do not require any special attention. On direct meta-analysis, only two placebo-controlled trials each of Adalimumab (OR 2.09 [95% CI: 1.34, 3.27]) and Ustekinumab (OR 1.79 [95% CI: 1.23, 2.58]) were included, and both biologics had a significantly superiority over placebo. Direct and network comparisons for induction CDAI-70 in TNF antagonist-experienced CD patients were similar, and the efficacy of Adalimumab was higher than that of Ustekinumab (Figure 5).

Figure 5. (A) SUCRA (the surface under cumulative ranking curve) values of each intervention in efficacy evaluations of induction therapy in tumor necrosis factor antagonist-experienced patients with moderate-to-severe Crohn’s disease. SUCRA values are expressed on a scale from 0 to 100. The closer the value is to 100, the more likely the intervention is to be among the most effective. Conversely, the closer the value is to 0, the less effective the treatment is likely to be. (B) League heat plots of mixed comparisons of inducing clinical response (defined by a reduction in the CDAI [Crohn’s Disease Activity Index] ≥70 [CDAI-70] or ≥100 [CDAI-100] points compared to baseline) between included biologic agents in tumor necrosis factor antagonist-experienced moderate-to-severe Crohn’s disease, reporting odds ratios on the logarithmic scale (log OR) with 95% confidence intervals. Log OR greater or less than 0 are indicated in red/yellow or blue/green, respectively, in comparisons of inducing CDAI-100/CDAI-70, and the darker the color, the greater the odds ratios. Bold type represents statistically significant superiority/inferiority of the intervention over the comparator.
In the evaluation of inducing CDAI-100 in TNF antagonist-experienced CD patients, all but Risankizumab (OR 2.55 [95% CI: 0.86, 7.60]) and Certolizumab Pegol (OR 1.30 [95% CI: 0.64, 2.62]) were significantly superior to placebo on direct meta-analysis. On network meta-analysis, Ustekinumab (SUCRA 86.19) and Risankizumab (SUCRA 62.56) were ranked highest (Figure 5).
3.4.2 Maintenance therapyOnly maintenance clinical remission was evaluated for TNF antagonist-naïve/experienced patients. A total of 5 RCTs including 866 TNF antagonist-experienced patients with moderate-to-severe CD evaluated maintenance clinical remission after treatment with Adalimumab (n = 1 trial), Ustekinumab (n = 2 trials), Vedolizumab (n = 2 trials, included one trial evaluating Vedolizumab SC).
In the evaluation of maintaining clinical remission in TNF antagonist-experienced patients, all agents were significantly superior to placebo on direct meta-analysis. On network meta-analysis, Adalimumab (SUCRA 80.09) and Vedolizumab (SUCRA 60.25) were ranked highest (Figure 4C).
3.5 Safety in overall patients with Crohn’s diseaseDue to the lack of safety subgroup analysis data on the medication history of TNF antagonist, only the safety of each biologic agents in overall CD patients was evaluated.
3.5.1 Induction therapyIn the safety evaluation of patient with moderate-to-severe CD in induction therapy, direct and network comparisons for risk of AEs, SAEs, or SIs in induction therapy were similar, with no statistical differences between any of the included interventions. On network meta-analysis, Risankizumab (SUCRA 84.81), Adalimumab (SUCRA 71.67), and Ustekinumab (SUCRA 52.64) had the lowest risk of AEs during induction therapy. Risankizumab (SUCRA 94.23), Adalimumab (SUCRA 74.72), and Ustekinumab (SUCRA 49.49) had the lowest risk of SAEs during induction therapy, and Risankizumab had a significant safety benefit over Ustekinumab, Vedolizumab, and Certolizumab Pegol. Risankizumab (SUCRA 79.73), Certolizumab Pegol (SUCRA 62.88), and Adalimumab (SUCRA 59.03) had the lowest risk of SIs during induction therapy (Figure 6A).

Figure 6. (A) SUCRA (the surface under cumulative ranking curve) values of each intervention in safety evaluations of induction therapy in overall patients with moderate-to-severe Crohn’s disease. SUCRA values are expressed on a scale from 0 to 100. The closer the value is to 100, the more likely the intervention is to be among the most safety. Conversely, the closer the value is to 0, the less effective the treatment is likely to be. (B) SUCRA (the surface under cumulative ranking curve) values of each intervention in safety evaluations of maintenance therapy in overall patients with moderate-to-severe Crohn’s disease. SUCRA values are expressed on a scale from 0 to 100. The closer the value is to 100, the more likely the intervention is to be among the most safety. Conversely, the closer the value is to 0, the less effective the treatment is likely to be.
3.5.2 Maintenance therapyIn the safety evaluation of patients with moderate-to-severe CD in maintenance therapy, there was no significantly difference between included interventions in evaluation of the risk of AEs on direct meta-analysis. In the SONIC trial (Infliximab vs. Infliximab combined with azathioprine), Infliximab alone (5 mg/kg maintenance regimen of Infliximab) had a significantly higher risk of SAEs than in combination with azathioprine (OR 1.77 [95% CI: 1.03, 3.05]), while the other comparisons between the agents were not significantly different. On network meta-analysis, IFX-10 (SUCRA 73.71), Vedolizumab SC (SUCRA 59.74), and RZB-180 (SUCRA 56.31) had the lowest risk of AEs during maintenance therapy. BI 695501 (SUCRA 97.58), Ustekinumab (SUCRA 71.48), Infliximab in combination with azathioprine (SUCRA 70.48) had the lowest risk of SAEs during maintenance therapy, and BI 695501 had a significant safety superiority over almost all of the other agents (except Ustekinumab and Infliximab in combination with azathioprine). Vedolizumab SC (SUCRA 84.59), RZB-180 (SUCRA 59.46), and IFX-10 (SUCRA 58.85) had the lowest risk of SIs during maintenance therapy (Figure 6B), and Vedolizumab SC had a significant lower risk of SIs compared to Certolizumab Pegol (log OR -2.22 [95% CrI: −4.42, −0.17]).
3.6 Sensitivity analysis and consistency analysisWe conducted several sensitivity analyses and the general consistency of the results confirms the robustness of our findings (all sensitivity analyses results are detailed in Supplementary File 2). In consistency vs. inconsistency plots, the contributions to the deviance are very similar and close to 1, indicating no evidence of inconsistency in our networks.
4 DiscussionIn this updated systematic review and Bayesian network meta-analysis, we combined direct and indirect evidence from 31 RCTs to evaluate the efficacy of different therapies for inducing and maintaining clinical remission or clinical response in moderate-to-severe CD populations. Several important findings from this network meta-analysis may inform clinical decisions. Firstly, two TNF antagonists, Infliximab and Adalimumab, continue to have a high status in induction and maintenance therapy. In addition, Infliximab in combination with azathioprine has a significant superiority in induction therapy in TNF antagonist-naïve patients, and appropriately increasing the dose of infliximab (10 mg/kg) may improve the efficacy of maintenance therapy. Secondly, Ustekinumab and Risankizumab may be the therapeutic agents of choice for TNF antagonist-experienced patients. High-dose Risankizumab (360 mg) also failed to show more efficacy benefits than low-dose Risankizumab (180 mg) in maintenance therapy. Thirdly, Vedolizumab does not offer superior therapeutic safety commensurate with its mechanism, and the subcutaneous injection formulation of Vedolizumab needs to demonstrate advantages beyond efficacy to establish its superiority over the widely approved intravenous infusion formulation. Finally, Risankizumab may be have worth-exploring lower safety risks in induction therapy. Altogether, these findings will inform the optimal sequencing of biologic therapy for patients with different histories of biologic administration.
Despite the emergence of new biologic agents, TNF antagonists remain most extensively experienced in the therapy of CD. In addition to the high-ranking performance in this network meta-analysis, TNF antagonists play a defined role in patients with fistulizing or structuring CD (Present et al., 1999; Sands et al., 2004; Bouhnik et al., 2018; Lee et al., 2018; Rodríguez-Lago et al., 2020), and seems to be a valuable option in the treatment of extraintestinal manifestations given the good response rates in a retrospective analysis of the Swiss IBD Cohort Study (Vavricka et al., 2017), though we acknowledge estimates supporting a large effect size for Infliximab have a low confidence due to the small number of induction RCTs available for inclusion and the small sample size of RCTs that were included. There was no statistically significant difference between 5 and 10 mg/kg intravenous infusion of Infliximab, which are both approved for the treatment of CD. However, in the three-arm ACCENT-1 trial, high-dose Infliximab (IFX-10) was associated with a superiority of SUCRA compared to the low-dose (IFX-5) in maintenance therapy (Hanauer et al., 2002). Combined with the fact that there is currently no evidence of higher safety risks associated with higher doses of Infliximab, this seems to suggest that increasing the dose of Infliximab has the potential to improve efficacy in maintenance therapy. While also as a TNF antagonist, Certolizumab Pegol did not show similar efficacy in the treatment of CD in this NMA. Nevertheless, in a retrospective analysis compared the real-world efficacy and safety of different TNF antagonists in biologic-naïve patients with CD, Certolizumab Pegol was comparable in efficacy to Adalimumab (Singh et al., 2016), and a head-to-head active-comparator RCT is required to judge the precise efficacy of Certolizumab Pegol.
Though the irreplaceable role of TNF antagonists in the treatment of CD, unfortunately one-third of patients with CD do not respond to initial treatment with TNF antagonists, and another one-third have only a transient response requiring a dose increase or switching to another therapy (Hanauer et al., 2002; Hanauer et al., 2006; Colombel et al., 2007; Sandborn et al., 2007a; Schreiber et al., 2007). Preventative combination treatment comes into view and may be the management of non-response. In our analysis, Infliximab in combination with azathioprine demonstrated clear efficacy benefit whereas Adalimumab in combination with azathioprine did not. In the SONIC trial, TNF antagonist-naïve patients with moderate-to-severe CD who received Infliximab in combination with azathioprine had a significant benefit on the rates of corticosteroid-free clinical remission compared to those receiving Infliximab alone or azathioprine alone, with comparable toxicity among groups (Colombel et al., 2010). In contrast, the open-label DIAMOND trial in which the efficacy of Adalimumab in combination with azathioprine did not differ significantly from that of Adalimumab monotherapy in patients naïve to both TNF antagonists and immunosuppression (Matsumoto et al., 2016). In both trials, patients receiving combination therapy who experienced worsening of CD were significantly fewer than those receiving TNF antagonist monotherapy (p = 0.045 in SONIC, p< 0.001 in DIAMOND, using Fisher’s Exact Test). This suggests that combination therapy may help prevent LOR to TNF antagonists, although LOR is not the only cause of worsening of CD (Ben-Horin and Chowers, 2011).
However, the populations of DIAMOND and SONIC were naïve to immunosuppressants and biologics, meaning that the effect of combination therapy in preventing LOR in immunosuppressant- and biologic-experienced patients remains unknown. Therefore, some researchers evaluated the benefit to risk ratio of concomitant immunosuppressives with scheduled TNF antagonists by identifying the influence of withdrawal of immunosuppressives. In an open-label interventional study reported by Van Assche G et al., there was no significant difference to continuation of immunosuppression in combination for < or = 6 months compared to scheduled Infliximab monotherapy in the proportions of patients with secondary non-response (Van Assche et al., 2008). Continuation of Adalimumab combined with oral thiopurines beyond 6 months offers no clear benefit over scheduled Adalimumab monotherapy in the DIAMOND-2 trial (Hisamatsu et al., 2019). Similarly, there is no evidence of superior efficacy of concomitant immunomodulating medication in therapy with non-TNF antagonistic biologics but come with an increased risk of SIs (Hu et al., 2021; Yzet et al., 2021). Overall, the role of concomitant immunosuppressives in treatment of CD still needs to be explored further.
In recent years, patents of Infliximab and Adalimumab have expired in many countries, and the huge biologics market has made biosimilar manufacturers eager. Both biosimilars, CT-P13 and BI 695501, were comparable in efficacy and safety to their respective originators in direct head-to-head comparisons (Ye et al., 2019; Hanauer et al., 2021). Subcutaneous injections formulation of CT-P13 (CT-P13 SC) is a product worthy of attention. The pharmacokinetics, as manifested by trough concentrations of the agents, increased after CT-P13 switching from intravenous to subcutaneous administration in a phase 1 study (Schreiber et al., 2021). Smith PJ et al. observed high treatment persistence rates and low rates of immunogenicity in IBD patients with maintenance therapy switching from Infliximab to CT-P13 SC in a multicenter retrospective cohort study (Smith et al., 2022). The results of the LIBERTY-CD trial demonstrate that maintenance therapy with CT-P13 SC provides both a robust clinical benefit and the convenience of subcutaneous administration to moderate-to-severe CD patients (Colombel et al., 2023).
In this network meta-analysis, although Adalimumab had the largest SUCRA value in the evaluations of inducing clinical remission and CDAI-70 in TNF antagonist-experienced CD patients, we recommend Ustekinumab and Risankizumab as the therapeutic agents of choice for induction therapy in TNF antagonist-experienced patients, because of the intransitivity caused by the inclusion criteria, which selectively included the patients with intolerance or secondary non-response to Infliximab, in the GAIN trial (Sandborn et al., 2007c). In contrast, the SEAVUE trial, a head-to-head trial to standard doses of different biologic agents for CD treatment, strengthens the reliability of our findings (Sands et al., 2022). The results of inconsistency analysis showed that there was no inconsistency between direct and indirect evidence of the comparison of Adalimumab and Ustekinumab (Dias et al., 2010; Dias et al., 2014b).
Notably, the high clinical benefit in SEAVUE compared to other RCTs may be attributed to several factors: the short disease course, the biologic-naïve baseline characteristics of enrolled patients (received early biologic treatment [EBT]), and non-placebo-controlled design (patients were aware they received active study therapy) (Sands et al., 2022). But in fact, the superiority of EBT over conventional therapy (CT) for CD is disputed. The result of an upgrade of a previous CADTH (Canadian Agency for Drugs and Technologies in Health) rapid response reported by Thompson W et al. suggested that the clinical effectiveness of EBT compared to
留言 (0)