The significance of the palmar skin in Dupuytren’s disease formation, propagation, surgical therapy, and recurrence risk, remains uncertain. Dupuytren’s disease patients can be treated with many different therapies. Only mild disorders of the disease can be observed. Collagenase injections intra-lesional, percutaneous needle fasciotomy, or selective aponeurectomy are all options, although progression or recurrence occurs in up to 85% of instances [10, 11].
Although up to 100% of patients have a recurrence, limited fasciectomy [12] is the most common treatment for moderate to severe conditions. Hueston [13] proposed skin replacement as a treatment for recurrent Dupuytren’s disease in the 1960s. Gonzalez [14] came up with this theory, emphasizing the need to remove all pre-axial tissue (skin, fat, and fibrous tissue) and replace the defect with a full-thickness skin graft (FTSG) [15, 16].
The same group later discovered fibromatosis in the skin of individuals with recurring Dupuytren’s disease, leading to the recommendation of dermo-fasciectomy as the best surgical choice [17]. Since then, studies have shown that dermo-fasciectomy and full-thickness skin grafts can reduce the incidence of recurrence by up to 33% [18, 19].
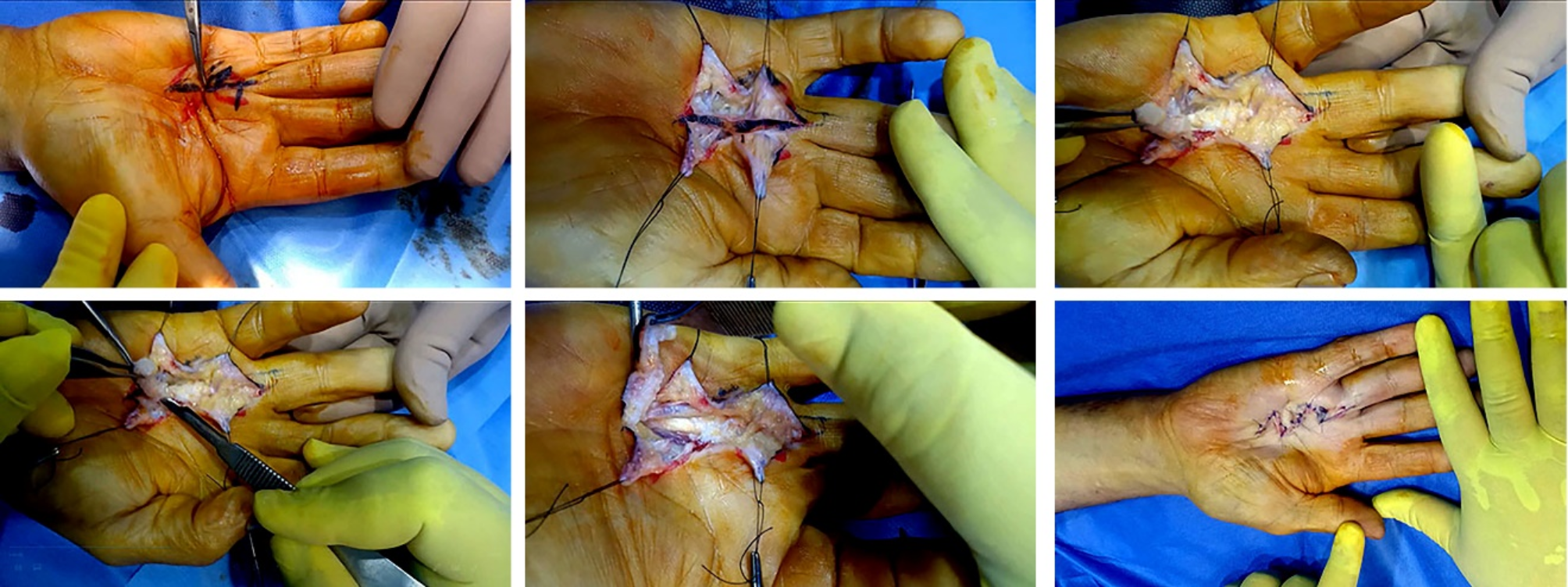
In our research, we removed 2–3 mm of adhering skin along with the entire cord. At the commencement of the cord, we also removed the adhering fascia. We did not remove any fascia beyond the natatory ligament since we found that there was a good subcutaneous layer under the cord and covering the fascia of the digits. In none of our situations has there been a recurrence. This is due to the fact that we assumed the disease-causing tissue was the skin rather than the fascia when we removed it.
There is limited literature comparing the clinical and histological features of Dupuytren’s disease in the skin [20] and there are no reports on microscopic examination of clinically uninvolved skin [14]. Wade et al. [21] discovered cutaneous fibromatosis in 61% of histopathological cases. In addition, 22 of the 44 patients with dermal involvement had no clinical symptoms of skin involvement and were treated with fasciectomy. This finding supports our hypothesis that Dupuytren’s illness begins in the dermis before progressing to fascia involvement and manifesting clinically.
All our specimens showed inflammatory lesions with hyperkeratotic epidermal covering and dermal infiltration with aggregation of chronic inflammatory cells, primarily lymphocytes, and plasma cells, proliferating vascular spaces, and fibrous stroma. There were no granulomas or malignant alterations found. This further supports our theory that this is a chronic inflammatory skin condition that begins in the deep dermis at stress points. Because the palmar fascia is very adherent to the dermis in the palm, it appears to originate there. However, as we have demonstrated clinically, the cord is separated from the fascia by a well-defined subcutaneous layer distally.
In limited/small skin biopsies, histologically distinguishing Dupuytren’s fibromatosis from hypertrophic scarring is not always achievable. Because the tissue in both circumstances has enhanced cellularity and fibroblastic activity, the morphological traits are identical. Hypertrophic scars, on the other hand, usually have thick collagen bundles and do not create “burned out” fibrotic nodules, which are common in late-stage Dupuytren’s disease [22], As a result, the general morphology plays a big role in the diagnosis. On the other hand, one could argue that distinguishing between dermal fibromatosis and excessive scarring is unnecessary because the most important task is to remove all fibrotic tissue, which is also the conclusion of our study, which found that this disease should be treated as strongly fibrotic scar tissue that passes over joints, which is why we have performed multiple z-plasty to prevent a recurrence.
Gonzalez [14] demonstrated that dermo-fasciectomy substantially excised skin, fat, fascia, aponeurosis, scar, and diseased tissue, resulting in a significant improvement in range of motion. However, they are unable to fully explain why their dermo-fasciectomy patients have straighter digits and advise that this is an issue that should be researched further. However, we can attribute this improvement to the fact that the disease began on the skin, which was completely removed, reducing the risk of recurrence.
Anecdotally, some surgeons discourage the use of dermo-fasciectomy due to the alleged risk of graft loss, perceived surgical complexity, and longer rehabilitation. To date, no studies have demonstrated a statistically or clinically significant risk of graft loss. According to anecdotal evidence, these patients take longer to resume normal daily activities, which should be balanced against a potentially lower rate of recurrence and revision surgery [23, 24]. We performed restricted surgery in our study, removing the chord and the adhering skin above it, and had great results with no recurrence. We do not have a skin graft; therefore, we’ve avoided all of the difficulties that come with them. Our patients began working one to two weeks after the stitches were removed.
The use of hand therapy in the treatment of Dupuytren’s disease has been recommended in numerous studies [25]. Hand therapy as a prophylactic treatment for Dupuytren’s disease has insufficient evidence. Hand physical therapy was individualized to each patient’s needs after corrective treatment and includes orthotics, exercise, edema control, and pain or scar management. Because we had limited surgery and did not touch the fibrous flexor sheath in our study, we did not refer our patients to the physiotherapy department.



留言 (0)