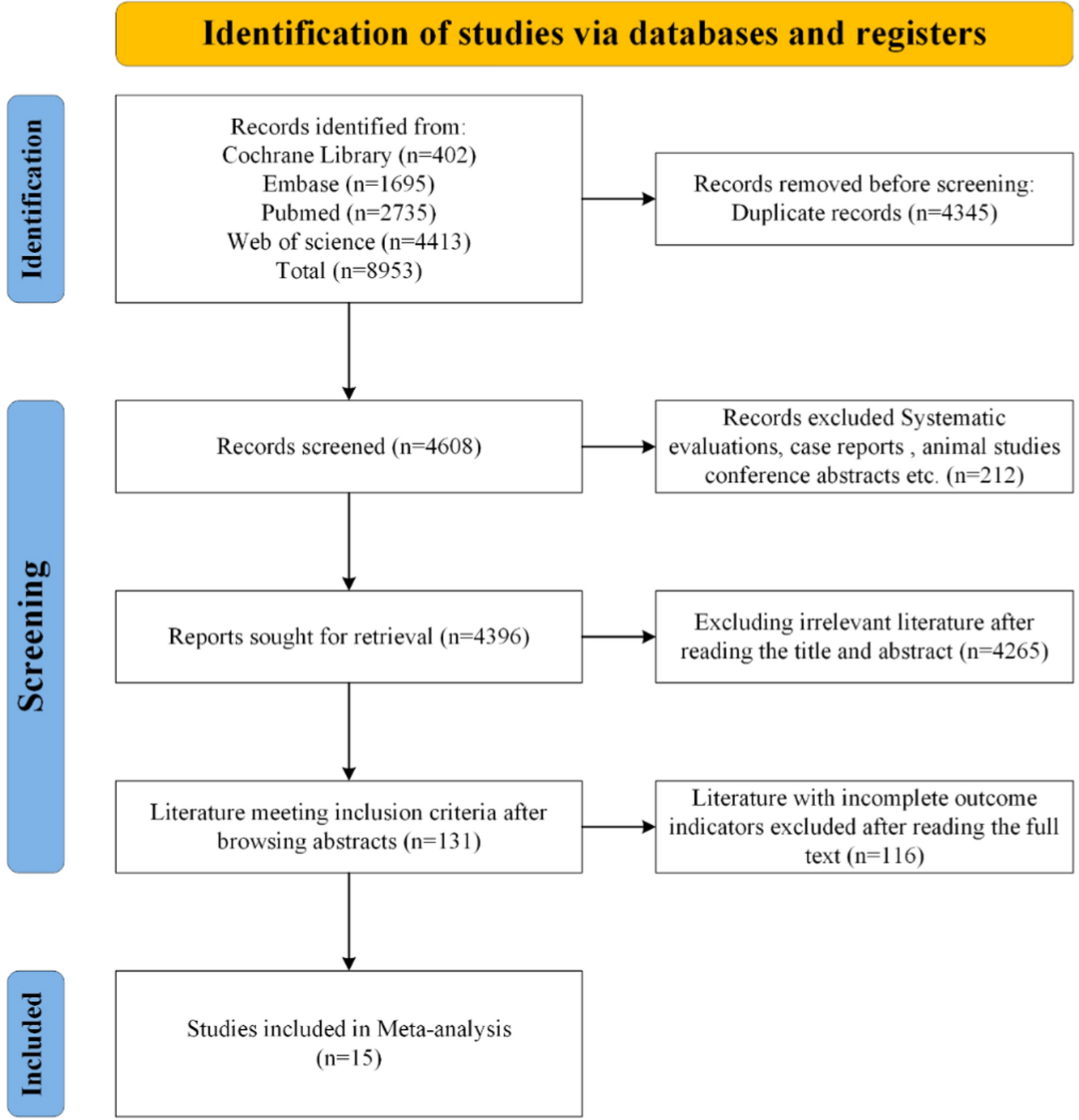
This meta-analysis included 15 cohort studies comparing the prosthetic survival and clinical outcomes of patients with unicompartmental osteoarthritis of the knee treated with lateral and medial UKA. The study involved 614 cases in the lateral UKA group and 2,592 cases in the medial UKA group.
The results indicated no statistically significant differences between lateral and medial UKA in terms of functional scores, pain scores, aseptic loosening, postoperative progression of contralateral arthritis, and prosthesis survival rates. This suggests that both treatment options achieve similar efficacy, consistent with a study by Filippo Migliorini in 2023 [19].
Although lateral and medial KOA present different pain patterns—lateral KOA often causes significant pain during knee flexion [32], while medial KOA results in pain during knee extension due to cartilage damage in the anterior and middle portions [33]. Both UKA types can restore the natural alignment and structure of the knee joint post-surgery [34]. Therefore, achieving similar postoperative scores in both groups is expected.
Regarding aseptic loosening, all cases in our study occurred in medial UKAs, consistent with Tay’s findings [35]. This study indicated that imprecise postoperative implant positioning in medial UKAs increases the likelihood of aseptic loosening [36, 37]. However, the authors concluded that imprecise implant positioning could equally affect both lateral and medial UKAs, resulting in no statistically significant difference in aseptic loosening between the two. The absence of aseptic loosening in the lateral UKA group may be due to the small sample size, suggesting a need for larger comparative studies.
For the progression of postoperative contralateral arthritis, it has been suggested that intraoperative overcorrection is a contributing factor [31, 38]. Tong Zheng recommended maintaining more than 3° of valgus alignment after lateral UKA [39] and 1°–4° of slight valgus for medial UKA [40,41,42] to achieve optimal functional outcomes and survival rates. However, overcorrection is typically related to surgical technique rather than the type of UKA, leading to no significant difference in contralateral arthritis progression between the two groups.
In this study, we found no statistically significant difference in postoperative prosthetic survival between the medial and lateral UKA groups. Both groups demonstrated high prosthetic survival rates: in the short- to intermediate-term, 96.0% in the medial group and 93.2% in the lateral group; in the long-term, 90.5% in the medial group and 90.3% in the lateral group.
The question of which prosthesis (medial or lateral UKA) has a better survival rate remains controversial. Some studies report higher survival rates for medial UKA, others for lateral UKA, while some suggest little difference between the two [18, 19, 26, 27]. Clinically, lateral UKA is used less frequently than medial UKA because the incidence of isolated lateral knee osteoarthritis is only one-tenth that of medial osteoarthritis [43]. Additionally, there are significant anatomical and biomechanical differences between the compartments: the lateral tibial plateau is convex, whereas the medial is concave [44]. As a result, implants and surgical techniques effective for the medial compartment cannot be directly applied to the lateral compartment [45, 46].
Surgeons typically have more experience and refined techniques for medial UKA. However, the authors suggest that the results of this meta-analysis may be attributed to improvements in the design of lateral UKA implants, enhanced surgical techniques, and better patient selection, leading to increased survival rates for lateral UKA prostheses.
Regarding improvements in implant design for posterolateral UKA, several advancements have been made, such as the introduction of cementless components and redesigned polyethylene (PE) bearings [47,48,49]. In a 2010 study [13], Pandit used a new domed tibial plateau implant, reducing the rate of active spacer dislocation to 1.7%, compared to 10% in a 1996 study [50]. By 2018, Walker et al. demonstrated that a lateral unicondylar prosthesis with a mobile spacer had a survival rate of 90.1% at three years and 85.0% at five years [51]. After switching to fixed spacers in 2020, Walker et al. reported 100% survival at two years in 51 patients [52], significantly improving lateral prosthesis survival.
Improved surgical techniques have also contributed. According to Forster et al [53], the posterolateral approach reduces the risk of medial patellar subluxation compared to the medial approach. Regarding the rationalization of indications for lateral UKA, Berend et al [54] identified complete lateral cartilage loss and correctable medial joint deformity on stress radiographs as reasonable indications for lateral unicondylar arthroplasty.
Conversely, the actual prosthetic survival rate of medial UKA is often lower than ideal due to high surgical volumes, varying clinician skill levels, and inconsistencies in surgical approaches and prostheses. In summary, the increased survival rate of lateral UKA and the decreased survival rate of medial UKA have resulted in similar survival rates for both.
Our meta-analysis addresses a critical issue in current clinical practice: the choice of total knee arthroplasty for patients with posterolateral KOA, driven by uncertainty about the outcomes of posterolateral UKA. This trend may negatively impact future practice by limiting opportunities for physicians to develop expertise in posterolateral UKA and restricting patient access to advanced techniques. We advocate for the integration of posterolateral UKA into routine clinical care.
Lateral UKA is emerging as a valuable tool for treating posterolateral KOA. Although our study shows that posterolateral UKA can achieve results comparable to medial UKA, further research is necessary to investigate the impact of factors such as spacer type and material on the efficacy of posterolateral UKA.
However, our study faced several limitations. There was significant heterogeneity in the pain score data, as indicated by high I2 values, likely due to different rating scales. Unfortunately, we couldn’t perform subgroup analyses because too few studies used the same scale. Additionally, the included studies were cohort studies, lacking randomized controlled trials, which provide a higher level of evidence. We did not control for confounders such as age, BMI, gender, spacer type, and prosthesis type. Using data from original publications might have introduced biases inherent in observational studies. Furthermore, the mean follow-up time varied across the studies, and some of the prosthesis types examined were outdated.



留言 (0)