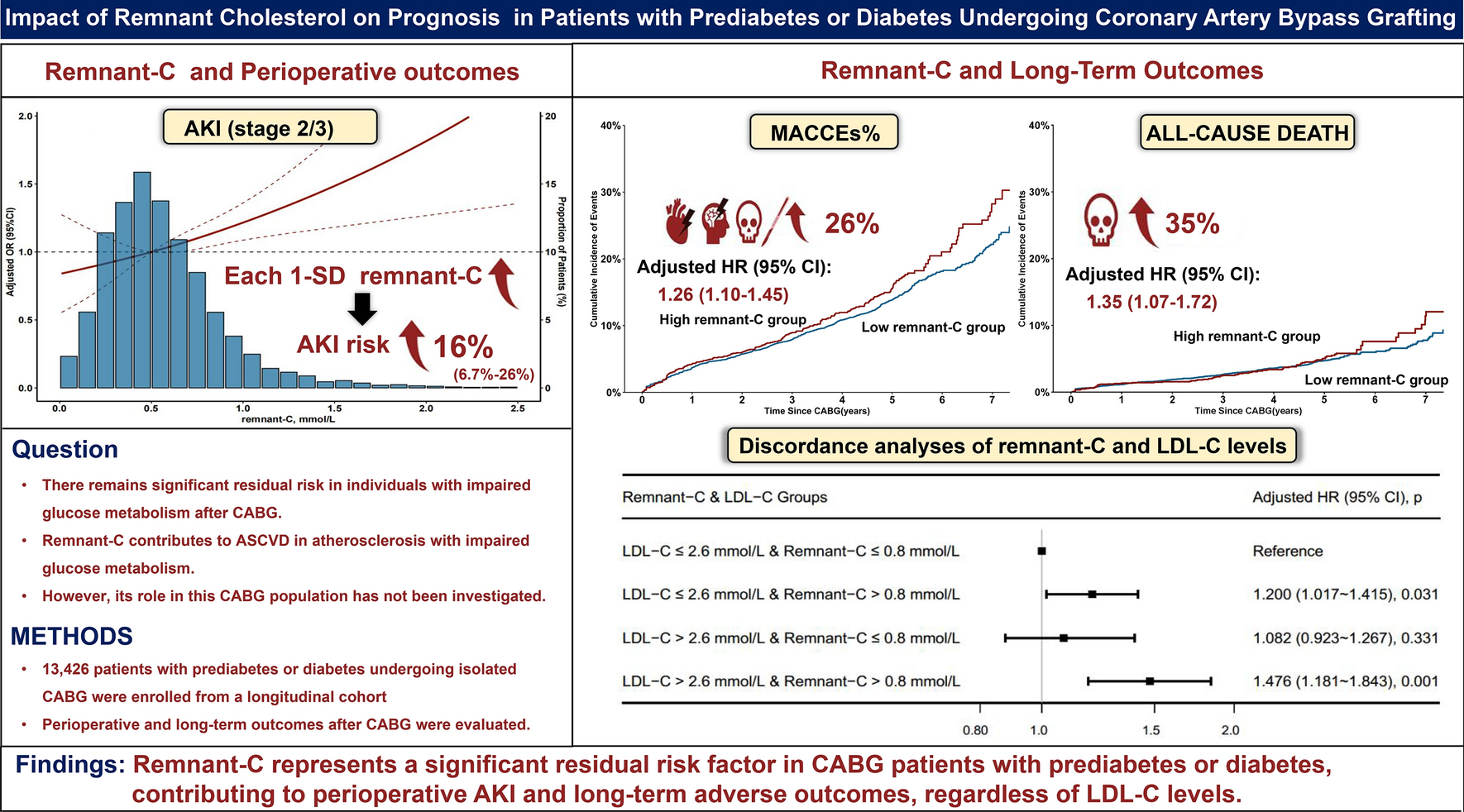
This large-scale cohort study is the first to demonstrate an association between elevated remnant-C and poor outcomes in patients with diabetes or prediabetes undergoing CABG. In the short term, elevated remnant-C was associated with an increased risk of perioperative AKI stage 2/3. Over the long term, elevated remnant-C was associated with a higher risk of MACCEs, all-cause mortality, MI, and repeat revascularization, and this association was more pronounced in insulin-treated patients compared to those not on insulin therapy. Furthermore, remnant-C is independently associated with MACCEs, regardless of LDL-C levels.
LDL-C is a well-established risk factor for ASCVD and a key target for both primary and secondary prevention. However, despite significant reductions in LDL-C, recurrent ASCVD events still occur in patients [8, 14]. Remnant-C has been shown to have a strong pro-atherogenic effect and may be an important contributor to this residual risk [4]. In individuals with impaired glucose metabolism, elevated remnant-C levels are observed, while LDL-C levels remain relatively normal [10]. A study found that elevated levels of remnant cholesterol are associated with poor glycemic control in individuals with diabetes, as assessed by continuous glucose monitoring devices [24]. Therefore, The residual risk associated with remnant-C in this population deserves special attention. Studies indicate that insulin resistance and pro-inflammatory states, prevalent in individuals with prediabetes or diabetes, not only promote remnant-C production but also amplify its cardiovascular impact [25, 26]. For CAD patients with impaired glucose metabolism, CABG is a key treatment, especially for those with multi-vessel disease [8, 13]. However, patients with diabetes or prediabetes undergoing CABG are at high ASCVD risk due to postoperative residual risk and underappreciated risk factors, which contribute to higher rates of both short- and long-term adverse events [27]. Notably, no studies have yet investigated the association between remnant-C and adverse outcomes in patients with impaired glucose metabolism undergoing CABG. This study is the first to explore this issue.
In the perioperative outcomes of this large longitudinal cohort of 13,426 patients undergoing CABG, we found that baseline remnant-C levels were significantly associated with AKI stages 2/3. Each 1-SD (0.4 mmol/L) increase in remnant-C was associated with a 16.6% increased risk of AKI after multivariate adjustment. This novel finding, for the first time, establishes a link between remnant-C and AKI after CABG. Prior studies have mainly focused on the impact of dyslipidemia on CKD. The Atherosclerosis Risk in Communities study showed that low HDL, high LDL-C, and elevated TG are linked to an increased risk of CKD [28], consistent with findings from large Mendelian randomization studies [29]. Additionally, in patients with diabetes, multiple epidemiological studies have confirmed that typical dyslipidemia strongly correlates with the incidence and progression of CKD [30]. However, few studies have investigated the relationship between blood lipids and perioperative AKI, with only limited observational evidence suggesting a modest association between HDL-C and AKI following both cardiac and non-cardiac surgeries [31, 32]. AKI is the most common major complication of cardiac surgery, occurring more frequently in patients with impaired glucose metabolism compared to those with normal glucose levels [33, 34]. Moreover, given the strong association between AKI, especially stages 2/3, and adverse outcomes, the management of AKI in cardiac surgery is a critical concern [34]. Our study demonstrates that remnant-C is associated with the occurrence of AKI Stage 2/3 in patients with diabetes or prediabetes undergoing CABG. This finding highlights the potential for remnant-C as a novel biomarker for early identification, risk stratification, and targeted clinical intervention. However, the mechanisms underlying the association between remnant-C and AKI remain unclear. Several hypotheses offer insights into potential pathways. First, the lipid nephrotoxicity hypothesis, which links dyslipidemia to CKD, suggests that persistent hyperlipidemia leads not only to atherosclerosis but also to glomerular arteriosclerosis [35]. Furthermore, the gradual accumulation of various circulating lipoproteins in the basement membrane and mesangial cells damages podocytes, mesangial cells, and renal tubular structures, promoting CKD progression [35]. Notably, in the context of impaired glucose metabolism, the renal microvasculature shows a unique susceptibility to dyslipidemia, which may be a key mechanism of renal injury [36]. Impaired glucose metabolism is often associated with insulin resistance and a pro-inflammatory state [25], both of which contribute to endothelial dysfunction. This dysfunction increases the permeability of renal microvasculature, promotes inflammation and oxidative stress, and alters renal microcirculatory hemodynamics [36, 37]. Moreover, in patients with impaired glucose metabolism, the elevated levels of various lipoproteins and lipids [38], particularly TRLs, further exacerbates inflammation and damage to the renal microvasculature, thus worsening glomerular injury and tubular-interstitial fibrosis, which ultimately accelerates the progression of kidney injury [36,37,38]. Meanwhile, the mechanisms related to remnant-C and cardiovascular events include the elevation of inflammatory cytokine levels, increased systemic oxidative stress, induction of endothelial dysfunction, and disruption of immune regulation [3, 4, 9, 25]. These mechanisms may also be involved in the development of AKI. In clinical practice, perioperative remnant-C/TG are often overlooked by physicians. Given our results, it is essential to further investigate the role of remnant-C in AKI after CABG, as well as to explore the underlying mechanisms.
Our study also revealed that elevated remnant-C has an impact on long-term clinical outcomes in patients with diabetes or prediabetes undergoing CABG. For each SD increase (0.4 mmol/L) in remnant-C, the risk of MACCEs increased by 6.6%, with corresponding increases of 7.1% in all-cause death and 11.2% in MI risk. Importantly, in this high-risk ASCVD group of patients with impaired glucose metabolism, remnant-C was identified as the primary cholesterol component driving MACCEs following CABG. Regardless of whether LDL-C levels were ≤ 2.6 mmol/L, patients with remnant-C levels ≥ 0.8 mmol/L had a higher risk of MACCEs, suggesting that remnant-C can predict cardiovascular outcomes independently of LDL-C levels. These findings support the consideration of remnant-C as both a clinical predictor and therapeutic target in patients with prediabetes and diabetes undergoing CABG. Current guidelines recommend long-term statin therapy for patients after CABG without contraindications [8]. However, the effect of statins on remnant-C is limited. A national longitudinal cohort study, involving approximately 2 million patients with diabetes, found that the association between remnant-C and cardiovascular disease was even stronger in those on statin therapy than in those not using statins [39]. A recent study suggest that lowering remnant-C by 0.8 mmol/L in secondary prevention can reduce the risk of recurrent MACCEs by 20% [11]. Based on these data, we reasonably postulate that treatment of residual risk, measured as remnant-C, was likely more beneficial than further reduction of LDL-C levels in patients with impaired glucose metabolism after CABG who are already receiving appropriate doses of statins. In fact, the effects of LDL-lowering drugs such as statins, ezetimibe and PCSK9 inhibitors on remnant-C levels are usually modest, while fibrates, commonly used in clinical practice to lower TG/TRL/remnant-C, have more profound effects [25]. In the PROMINENT trial [40], pemafibrate significantly reduced TG levels by 26.2% and remnant-C levels by 25.6% in patients with diabetes, but these changes did not translate into a reduction in MACCEs. Further analysis revealed that pemafibrate did not truly reduce remnant-C, but instead promoted its conversion to LDL-C rather than hepatic clearance. Consequently, pemafibrate-mediated reductions in remnant-C were accompanied by a 12.3% increase in LDL-C levels in this study [40]. Ongoing trials involving novel agents, such as RNA-based therapies targeting apolipoprotein C-III, angiopoietin-like protein 3 (ANGPTL3) inhibitors, protein-level interventions targeting ANGPTL3, and gene-editing therapies like CRISPR-Cas-mediated ANGPTL3 modification, are expected to improve the clearance of remnant-C rather than converting it to LDL particles, thereby reducing the atherogenic effects of remnant-C [15, 41, 42]. Moreover, selecting the appropriate patient population for remnant-C-lowering therapies is essential. Theoretically, patients with higher residual risk driven by remnant-C are more likely to benefit from these therapies. In our study, we specifically focused on patients with diabetes or prediabetes undergoing CABG, who represent a group with particularly high residual cardiovascular risk [13, 14, 27]. Therefore, our findings provide valuable insights into the selection of patient groups for remnant-C-lowering therapies.
In addition to the primary findings, our subgroup analysis revealed an interesting observation: the association between remnant-C and MACCEs was more pronounced in patients receiving insulin therapy compared to those not on insulin. Insulin-treated patients often have a longer duration of diabetes and more severe insulin resistance [43, 44]. Additionally, exogenous insulin acts as a pro-inflammatory agent, potentially exacerbating inflammatory responses through multiple mechanisms [44, 45]. This heightened insulin resistance and inflammatory state may amplify the effects of remnant-C on cardiovascular risk [25, 44]. In particular, exogenous insulin may enhance immune responses associated with inflammation and overstimulate hormonal signaling pathways, which could increase the uptake of remnant-C by macrophages in arterial walls, thereby accelerating the progression of atherosclerosis [45, 46]. This finding emphasizes the importance of paying more attention to the subgroup of insulin-treated patients with diabetes undergoing CABG, as these patients may be more vulnerable to the adverse effects of remnant-C.
The strengths of this study are as follows: it is based on a large-scale, well-validated longitudinal cohort with complete follow-up, and adequate adjustment for confounding factors, which together contribute to the robustness of the findings. Moreover, LDL-C was directly measured via the homogeneous method rather than estimated via the Friedewald equation. Both HDL-C and TC were also directly measured. Consequently, the remnant-C level, calculated as TC − HDL-C − LDL-C, provided a more accurate estimation. However, this study has several limitations. First, epidemiological and genomic studies have confirmed ethnic and regional variations in lipid profiles and associated cardiovascular risks [47, 48]. Given that this study is based on a Chinese population, the generalizability of its findings to other regions and ethnicities may be limited. Second, during long-term follow-up, remnant-C levels may fluctuate over time, but these fluctuations are difficult to track. Third, although we adjusted for known major covariates, the potential of residual or unmeasured confounding factors remained. Data on unmeasured confounders, such as patient lifestyle behaviors (e.g., diet, physical activity, alcohol consumption) and adherence to prescribed treatments, were not available during the follow-up period. These factors may contribute to cumulative exposure and variability in remnant-C levels, potentially influencing the observed associations between remnant-C and outcomes [49]. It is well established that socioeconomic status is closely related to the management, complications, and prognosis of diabetes, and it may also influence the observed associations in our study. Additionally, the lack of data on the duration of diabetes and its related complications further limits the comprehensiveness of our multivariate model, which may affect the interpretation of the results, particularly in the subgroup analysis involving insulin treatment. Finally, due to the inherent limitations of the observational study design, although we employed various statistical methods (e.g., restricted cubic splines, logistic regression, and Cox models) to ensure the reliability of the results, we acknowledge that confounding factors cannot be fully eliminated. Therefore, a causal relationship between remnant-C and MACCEs cannot be definitively established due to the potential influence of confounding and reverse causation.




留言 (0)