
記住我


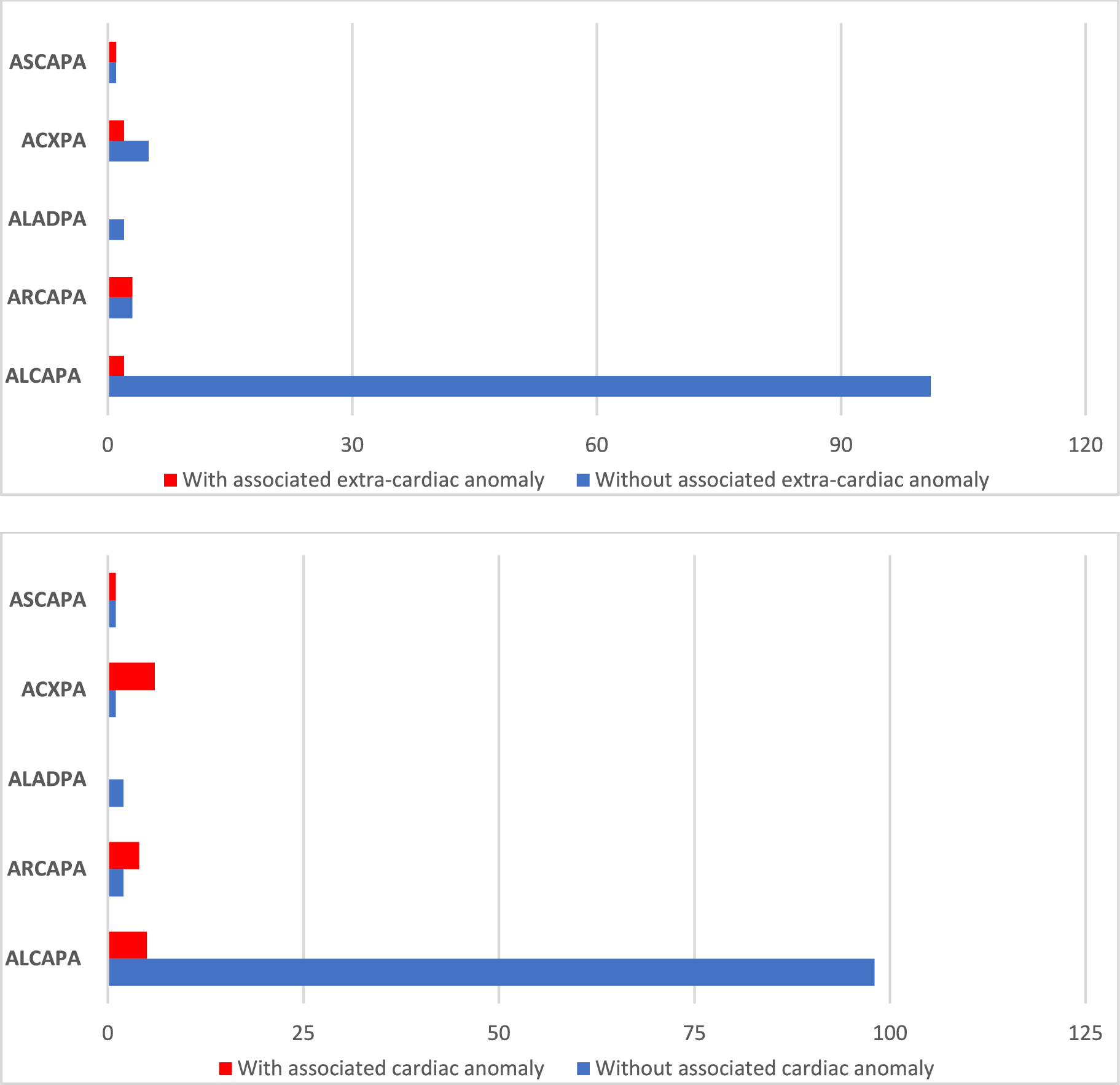
A total of 120 patients were included in the study, comprising 77 female (64%) and 43 male (36%). The diagnostic groups within the cohort exhibit a highly uneven distribution: 103 patients with ALCAPA (86%), 6 with ARCAPA (5%), 2 with ALADPA (1.5%), 7 with ACXPA (6%), and 2 with ASCAPA (1.5%) (Fig. 1).
Fig. 1
Overview of the distribution of associated cardiac and extra cardiac anomalies in patients with abnormal coronary artery from the pulmonary artery
ACAPA was diagnosed prior to surgery in 115 patients. In two patients, the coronary anomaly was discovered during the initial cardiac surgery for other congenital heart defects (one patient with Shone complex and one patient with hypoplastic left heart syndrome—HLHS), in 3 patients it was diagnosed postoperatively via cardiac catheterization (2 patients with aortic coarctation and one patient with Scimitar syndrome). Six patients did not have a surgical repair. A conservative approach without surgical intervention was chosen for patients in advanced stages of the disease, considering the anticipated poor prognosis and advanced age. Also, the presence of adequate coronary collateralization and satisfactory ventricular function supported the decision for a conservative approach. Consequently, in two patients for whom a corrective operation was considered but ultimately not performed, both echocardiography and cardiac catheterization were conducted. One of these two patients exhibited an anomalous origin of the right coronary artery from the pulmonary artery, which, due to sufficient collateralization, resulted in only minimal impairment of right ventricular function.
Pulmonary Artery ConnectionThere is a significant difference among the diagnostic groups regarding the location of the coronary artery connection to the pulmonary artery (p < 0.001). Notably, ACXPA patients frequently (6 out of 7 cases) have a connection to the right pulmonary artery. In total, 12 patients have a coronary artery connection to the right pulmonary artery, while only two patients have a connection to the left pulmonary artery. An overview of the location of the coronary artery connection to the pulmonary artery according to the subtypes is given in Table 1.
Table 1 An overview of the location of the coronary artery connection to the pulmonary artery according to the subtypesAssociated Cardiac AnomaliesPatients in the ARCAPA, ACXPA, and ASCAPA groups more frequently had associated cardiac defects (p = . < 001), compared to patients with ALCAPA, as shown in Fig. 1. Specifically, 5 of 103 ALCAPA patients (5%), 4 of 6 ARCAPA patients (67%), 6 of 7 ALCXPA (86%) patients and one of two ASCAPA patients had further congenital heart defect (Fig. 1).
Among patients with associated cardiac defects, left heart obstructions or shunt-lesions were most commonly observed. Only one patient had pulmonary valve stenosis, and there were no other right heart obstructions.
The accompanying cardiac defects included: Aortic coarctation (n = 8), bicuspid aortic valve (n = 2), ventricular septal defect (n = 6), atrial septal defects (n = 9), patent ductus arteriosus (PDA) (n = 5), aortic stenosis (n = 2 cases), aortic arch anomaly (n = 1), hypoplastic left heart syndrome (n = 2), left persistent superior vena cava (n = 3), aortopulmonary window (n = 1), Scimitar syndrome (n = 1), transposition of the great arteries (n = 1), pulmonary valve stenosis (n = 1). An overview of the individual associated cardiac anomalies is provided in Table 2.
Table 2 Overview of the patients with anomalous coronary arteries from pulmonary artery in relation to associated cardiac and extracardiac anomaliesAssociated extracardiac anomaliesIn the ALCAPA group, there was one patient with a pelvic kidney, one patient with Rubinstein-Taybi syndrome, and two patients with Scimitar syndrome having hypoplasia of the right lung. In the ARCAPA group, there was one patient with fetal alcohol syndrome, one patient with Goldenhar syndrome, and one patient with VACTERL association with hearing impairment. In the ALADPA group, there were no patients with extracardiac malformations. In the ACXPA group, there was one patient with pulmonary hypoplasia and one with cystic renal dysplasia combined with a vertebral body malformation. In the ASCAPA group, there was one patient with a diaphragmatic hernia. An overview of the extracardiac anomalies for each patient with the associated coronary anomaly is given in Table 2.
Patients with associated cardiac anomalies more frequently have extracardiac malformations (p < 0.001) and are more likely to have a connection to the right pulmonary artery (p < 0.001) than patients without associated cardiac anomalies, as shown in Table 3.
Table 3 Overview of the association between cardiac and extracardiac anomalies with the location of the connection between coronary artery and pulmonary arteryClinical OutcomesPerioperative mortality, defined as any death occurring within 30 days after surgery, occurred in 12 patients. Eight of these 12 patients had ALCAPA without another associated cardiac defect and one patient had associated VSD and CoA. All nine patients had their surgery before 1992. Among the other three patients, who died perioperatively from the later era, two patients had ASCAPA. One of them also had aortic coarctation and died 6 days after the surgery due to coronary ischemia and the other one died on the operating table during the second coronary surgery. One further patient had ALCAPA with aortic coarctation, small left heart structures and Scimitar syndrome. In this patient the diagnosis of ALCAPA was made after the initial coarctation surgery by persisting unstable hemodynamic situation. Even after surgical treatment of ALCAPA and pulmonary veins, the patient died due to circulatory failure.
留言 (0)