Our results suggest that despite successful treatment of psoriasis with five different therapies, including three biologics, patients still exhibited a residual inflammatory imprint characterized by elevated disease-specific cytokines compared to control subjects. In contrast, non-specific inflammatory markers showed no significant differences compared to the control group, suggesting that non-specific inflammation decreases and normalizes with successful treatment. The residual disease-specific cytokines correlated with patients’ BMI and waist circumference. These results shed additional light on the treatment-related changes in inflammation and could be clinically relevant.
We investigated systemic inflammation by measuring two types of inflammatory markers (non-specific and disease-specific) in young patients with psoriasis who were successfully treated with five different types of treatment (topical therapy, methotrexate, adalimumab, secukinumab, and guselkumab). Given the significant burden of cardiovascular disease and metabolic disease, to which systemic inflammation can be a major contributor, it is important to know whether successful treatment of psoriasis reduces systemic inflammation and cytokines that are present in both atherosclerosis and psoriasis, such as IL-17 [12]. In addition, although this is only speculation, residual inflammation may contribute to the recurrence or worsening of psoriasis after discontinuation of successful treatment. Overall, residual inflammation is a topic that has not yet been extensively studied, and its clinical relevance remains to be clarified. We studied residual inflammation in a wide range of patients, reflecting the real-life situation in which patients differ in terms of disease severity and duration, as well as treatment modalities. To our knowledge, this is the first study to investigate residual non-specific and disease-specific inflammatory markers in successfully treated young patients with psoriasis, treated with five different treatments at a stable disease stage. We found that disease-specific inflammatory markers were elevated in successfully treated patients. Among several markers, the following were elevated: IFN-γ, TNF, IL-1β, IL-12p70, and IL-17, while only the levels of IL-23 were comparable to those of the control group. The reason for the difference between IL-23 and other disease-specific markers is unclear. Another observation also deserves attention: the residual levels of disease-specific cytokines in patients treated with topical agents and methotrexate were surprisingly similar to those in patients treated with biologics. Regarding the separate groups, we found only a few individual, and not generalized, differences. Except for IL-23, levels of other cytokines targeted with biologics (TNF, IL-17) were also similarly elevated in patients treated with specific antibodies or with another treatment. We found that all disease-specific inflammatory markers correlated with BMI and waist circumference. Increased IL-17 levels in the secukinumab group compared to other patient groups could be due to IL-17 bound to secukinumab, although this was not explicitly measured. In addition, males had slightly higher levels of all six cytokines measured compared to females. We cannot provide an explanation for this result.
There is data on circulating inflammatory markers in psoriasis, but, specifically, residual inflammation in successfully treated patients has not been studied. It is known that inflammatory markers are elevated in psoriasis patients. Some studies investigated the presence of several disease-specific inflammatory cytokines such as TNF [13], IL-1β [7], IL-17A [14, 15], IL-23 [15], and other cytokines in patients with psoriasis, which were elevated compared to controls. A recent systematic review and meta-analysis found that IFN-γ, TNF, IL-2, IL-6, IL-8, IL-18, IL-22, chemerin, lipocalin-2, resistin, sE-selectin, fibrinogen, and C3 were elevated in patients with psoriasis compared to healthy controls, while IL-1β, IL-4, IL10, IL-12, IL-17, IL-21, IL-23, visfatin, and omentin were not significantly different in patients with psoriasis compared to controls [16]. Another recent meta-analysis, which summarized data from several small studies showed that among numerous inflammatory markers, elevated serum concentrations of the inflammatory cytokines IL-2, IL-17, IL-18, and IFN-γ are present in untreated psoriasis patients [17]. Conflicting results have been reported on the serum concentration of IL-17 in psoriasis patients. While some studies found elevated levels [18,19,20], others found no difference compared to healthy controls [21, 22]. Other studies have shown that disease-specific inflammatory markers correlate with disease severity, which is primarily measured by the PASI [8, 10, 23]. Overall, disease-specific inflammatory markers were mainly determined to investigate the correlation with psoriasis severity and/or as markers of treatment efficacy. Regarding non-specific inflammatory markers, it has been shown that hs-CRP is elevated in psoriasis patients and that hs-CRP serves as a marker for subclinical atherosclerosis in psoriasis patients [24, 25]. Again, the measurements were performed in different patient groups and clinical scenarios than in our case and could not be extrapolated to residual inflammation.
Our results indicate that although non-specific inflammatory markers are effectively reduced by treatment, disease-specific markers persist. The persistence of disease-specific markers may indicate that the skin response to treatment, as measured by the PASI, does not fully reflect the extent of systemic inflammation. On the other hand, this persistent inflammatory imprint could also explain, at least in part, the chronic and recurrent nature of psoriasis. Previous research suggests that the chronic and recurrent nature of psoriasis may be due to local immunologic memory on the skin, driven by tissue-resident memory T cells [26]. Our results suggest that in addition to local immunologic memory, residual disease-specific systemic inflammatory activity may also play a role in disease recurrence. Thus, our results support the prevailing hypothesis that biologic therapy is highly effective but only suppresses the activity of pathogenic immune cells without eradicating them [27]. Our results emphasize the potential role of overweight in residual inflammation. Indeed, disease-specific inflammatory markers correlated with BMI and waist circumference. This could be related to the inflammatory activity of adipose tissue, which secretes pro-inflammatory cytokines such as TNF, IL-1, and IL-6, which could further exacerbate systemic inflammation that overlaps with psoriasis [16, 28]. At this point, we can only speculate about the explanation. However, the clinical value of this observation needs to be investigated in a study examining the role of weight reduction in reducing residual inflammation [29]. In any case, this observation reflects the relationship between psoriasis, systemic inflammation, and excess body fat/weight. There is no doubt that psoriasis and obesity are closely intertwined [16, 28].
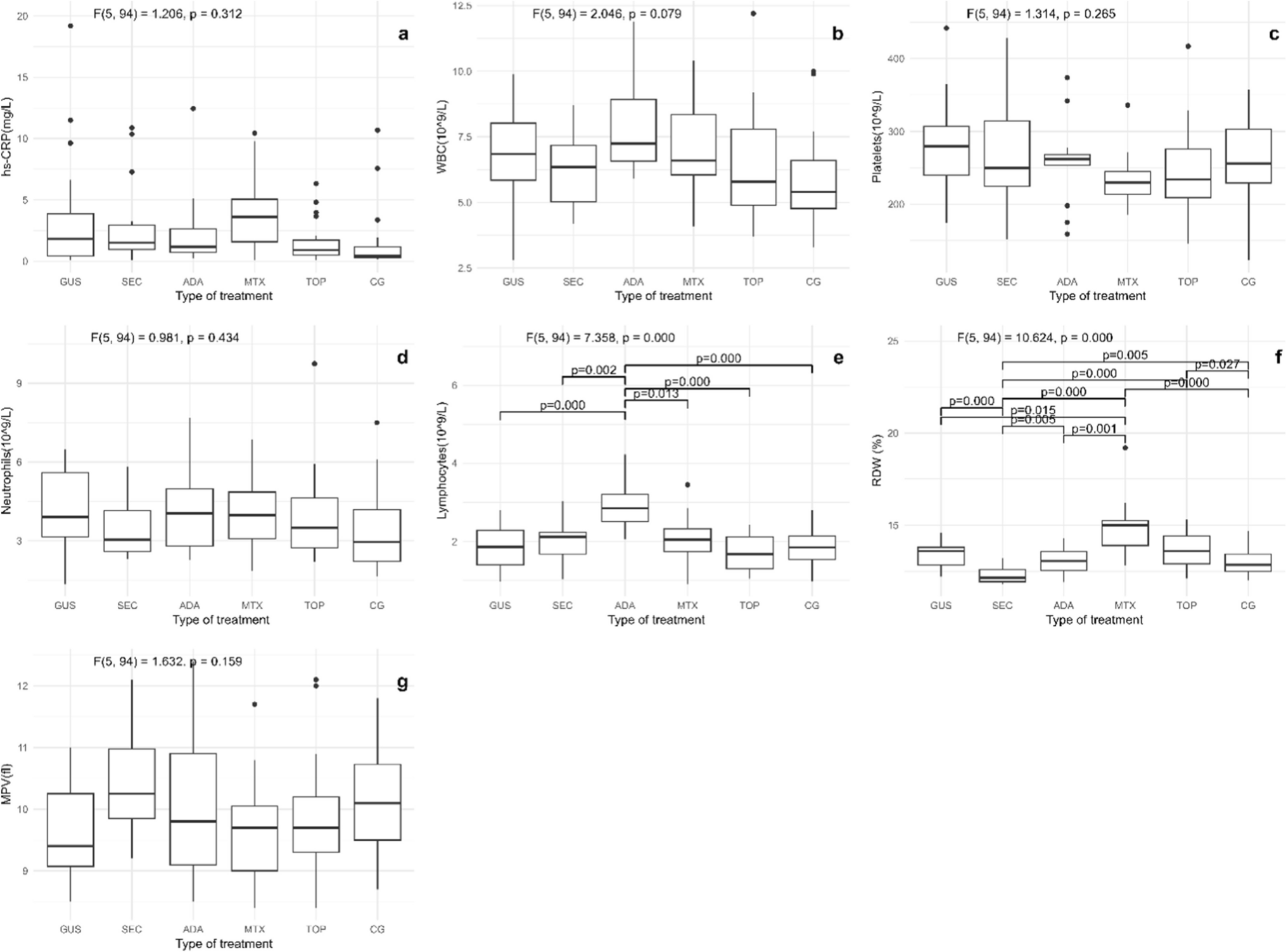
We have also investigated novel CBC-derived inflammatory markers that have been shown to be useful cardiovascular risk markers in patients with psoriasis [29,30,31]. It was shown that NLR and PLR decreased after treatment with TNF inhibitors [32, 33]. These markers did not differ significantly in the patient groups or the control group, suggesting that cardiovascular risk is not increased in successfully treated patients compared to the control group. This could indicate that the persistence of disease-specific inflammatory markers, which are also involved in the pathogenesis of atherosclerosis [29, 30, 34], does not significantly increase the cardiovascular risk after successful treatment. On the other hand, CBC-derived inflammatory markers may not be a suitable tool to assess cardiovascular risk in successfully treated psoriasis patients. Nevertheless, more data are needed to draw definitive conclusions because there are so many factors that influence cardiovascular risk in psoriasis patients, which may even differ in different clinical scenarios and still need to be clarified. Our results also showed that there was an inverse correlation between the duration of treatment and BMI in the psoriasis groups. These results emphasize the need for concurrent treatment of psoriasis and excess body fat/weight.
Our study has several limitations. The lack of previous data on inflammatory markers before initiation of therapy is a limitation of the cross-sectional study. However, we did not focus on the inflammatory changes before and after treatment, but on their levels in the stable phase of the disease. Another limitation was the relatively small number of patients in each group. However, similar results in three groups of patients treated with biologic therapy support the credibility of the results and conclusions.


留言 (0)