
記住我

To address the issue of small sample size and improve the generalizability of the trained model, we performed feature reduction. This involved eliminating less significant features. Feature reduction offers several benefits: faster training, reduced model complexity, improved model accuracy, and lower overfitting. For classification, as mentioned before, we chose a linear method (Elastic Net) and a non-linear method (Random Forest Classifier) to investigate their impact on the final results. After selecting the most important features, we used nested k-fold (k = 5) cross-validation with a grid search algorithm on the training set to identify optimal hyperparameters for both the Random Forest Classifier (RFC) and Elastic Net (EN). These hyperparameters included the number of trees in the forest (n-estimators), the maximum number of features to consider when searching for the best split (max-features), a constant that multiplies the penalty terms (α), and the Elastic Net mixing parameter (l1-ratio) for EN. After evaluating a range of reasonable values for these parameters, we found that the optimal parameters for the best estimator were n-estimators = 200, max-features = 2, α = 0.01, and l1-ratio = 0.9. Training accuracy for different hyperparameter values is shown in Table 1, and Table 2 for ElasticNet and RFC respectively. Setting max-features to 2 automatically triggers the code to run with a vector containing three parameters: [“auto”, “sqrt”, “0.2”]. The best accuracy with these parameters will be reported. After completing feature selection hyperparameter optimization, we trained our model using the original training data. The results were not as satisfying as we expected, so we applied data augmentation to the training data. We trained our model using augmented data to improve the classification accuracy. For classification, we employed an RFC, a supervised learning algorithm consisting of multiple decision trees trained independently with different samples. The RFC algorithm aggregates the predictions of these trees to make a prediction. The RFC algorithm selects random samples from the dataset, builds a decision tree for each selected sample, aggregates the prediction of this tree by voting (selecting the most frequent prediction). Finally, the algorithm determines the voted prediction as the final prediction. Figure 3 provides a visual representation of the RFC implementation.
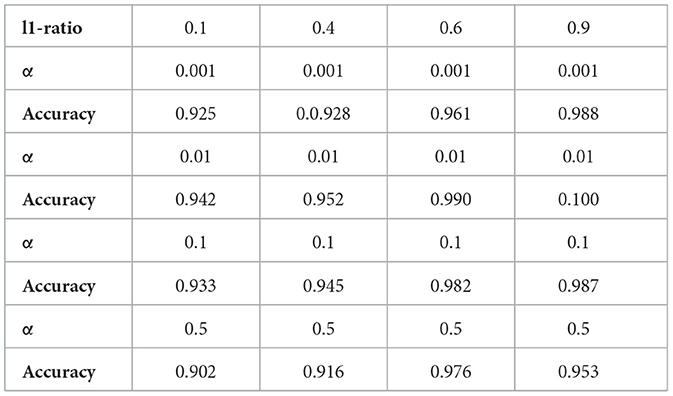
Table 1. Elastic net; mean training accuracy for different hyperparameter values.
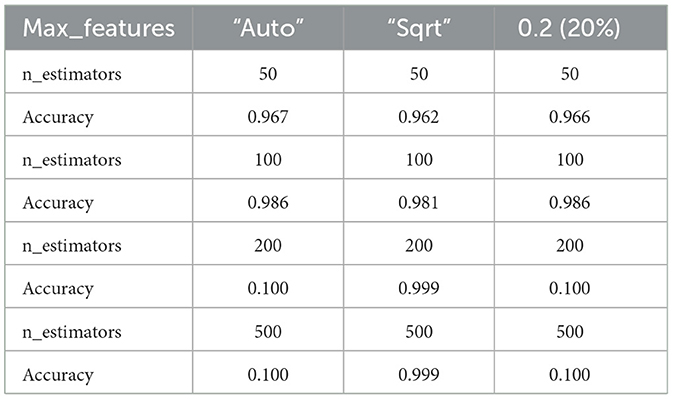
Table 2. RFC; mean training accuracy for different hyperparameter values.
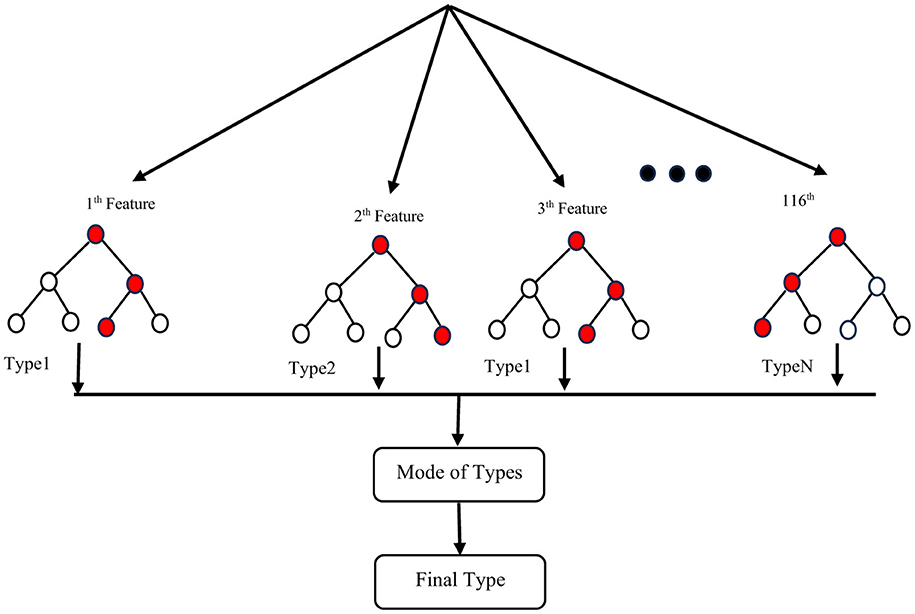
Figure 3. Implementation of an RCF.
Dataset [80 participants from a total of 96 (16 samples separated for test and validation from the original data)].
In addition to the RFC, we employed the EN as an embedded method. The EN combines the advantages of both wrapper models, which interact with the classification model, and filter models, which are less computationally intensive than wrapper models. This regularized regression method linearly combines L1 and L2 penalties, drawn from the LASSO and Ridge algorithms during training. We used the penalty parameters obtained through feature selection to select the most important features. The overlapping features between Sequential Floating Backward Search (SFBS) and Elastic Net were fed into a Python implementation of an EN classifier to distinguish between the three groups.
The ruling formula for this algorithm is illustrated in Equation 8 (Zou and Hastie, 2005).
θ^=argminθ(||y−Xθ||2+λ2||θ||2+λ1||θ||1) (8)where
||θ||1=∑i=1p|θi|and||θ||2=∑i= 1pθi2 (9)To have the best model we need to choose best weights that makes our predicted data with its coefficients similar to the observed data as much as possible. So according to the formula (Equation 8) we try to minimize loss function Ô by making Residual Sum of Squares (||y − Xθ||2), L2 Penalty (λ2||θ||2) and L1 Penalty (λ1||θ||1) as small as possible.
Considering α as λ2λ1+λ2, and λ1 as l1_ratio we will have the following formula which applicable in python:
θ^= argminθ(‖y−Xθ‖2+α.[(1−l1_ratio)]‖θ‖2 +l1_ratio‖θ‖1) (10)Solving Equation 8 will solve the optimization problem, and the total Elastic Net penalty would be:
ElasticNetPenalty=(αL1Penalty+(1−α)L2Penalty) (11)Figure 4 shows a schematic for steps showing how an EN is applicable on a dataset.
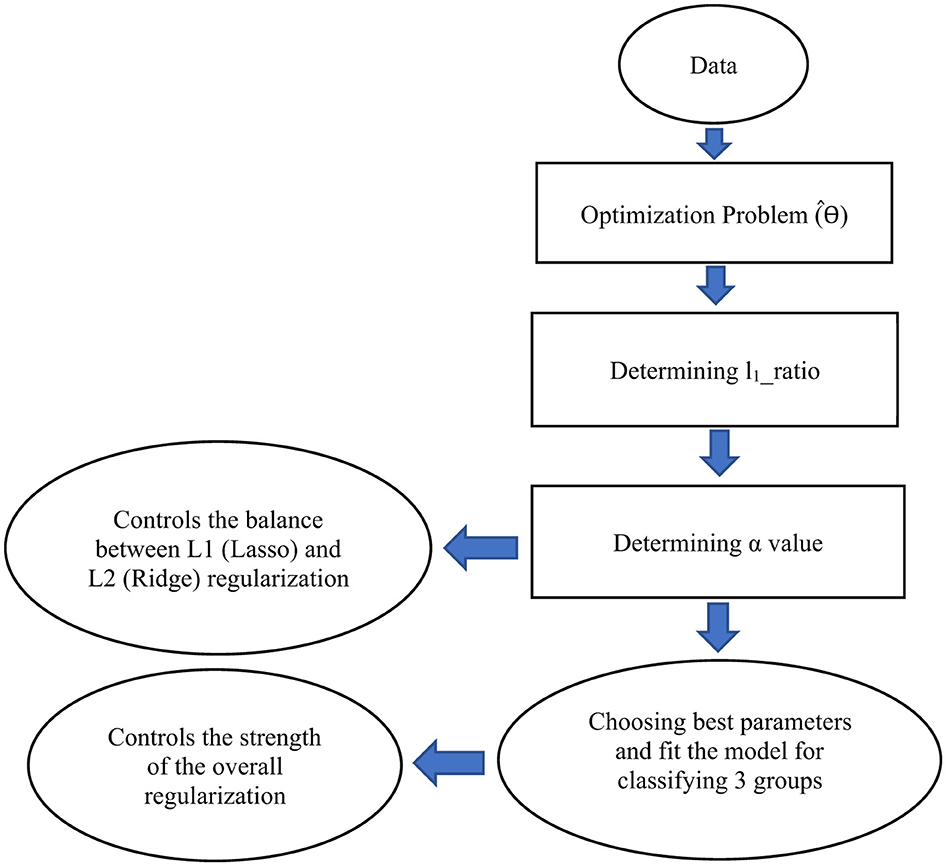
Figure 4. A schematic illustrating the steps to develop an Elastic Net (EN) model for classifying three groups. This schematic represents only the architecture of the EN framework. In our study, we combine Sequential Feature Backward Selection (SFBS) with EN to identify the optimal set of features for classification. EN has been implemented as a classifier not just as a regularization model. For this purpose, it can be implemented as a LogisticRegression with the option penalty = “elasticnet” in python.
Lastly, to estimate the classification accuracy, we calculated the error rate. We permuted the selected features randomly 10,000 times to obtain an empirical distribution of the average difference (p < 0.05).
Figure 5 shows a general schematic outlining the steps for data preparation leading to the final results.
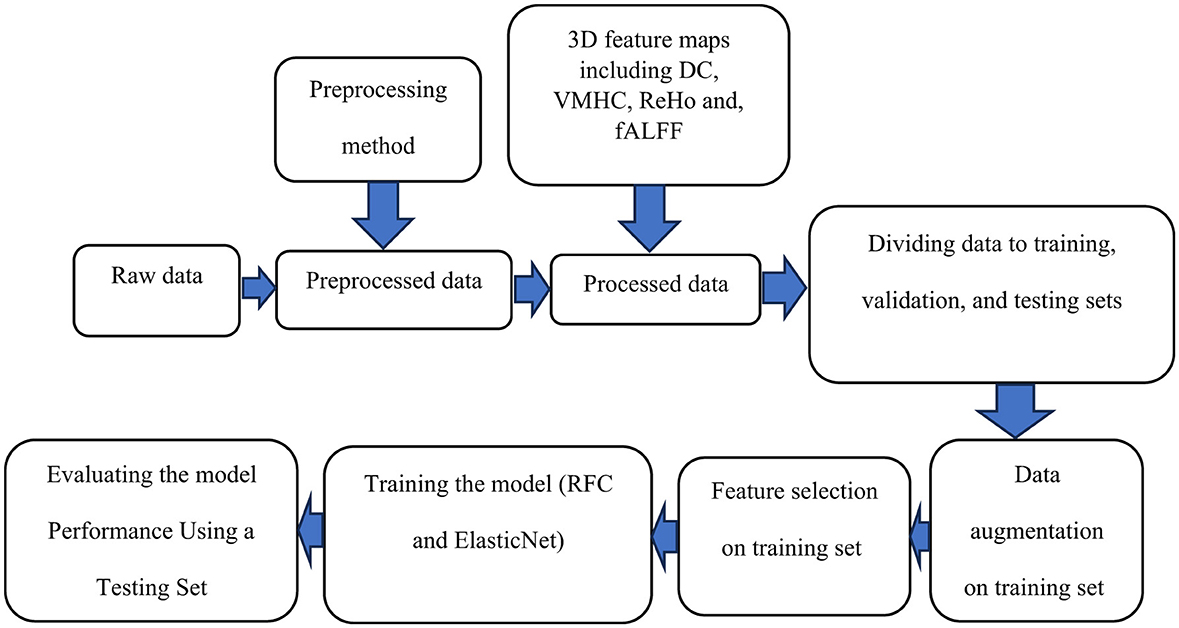
Figure 5. A schematic outlining the steps for data preparation and processing is shown. Initially, raw data undergoes preprocessing. The preprocessed data is then used to compute voxel-based connectivity measures, which serve as features for training. To enhance the model, data augmentation is applied to the training data, followed by feature selection. The model is trained using these features and evaluated with a test dataset. Finally, the results are reported.
3 ResultsTable 3 shows the demographic, clinical, and behavioral characteristics of the three groups (MDDs with suicide ideation, MDDs without suicide ideation, and healthy controls). The suicide ideators, non-suicide ideators, and HCs were well-matched in terms of age and education level. There was no significant difference in HDRS scores between MDDs with and without SI.
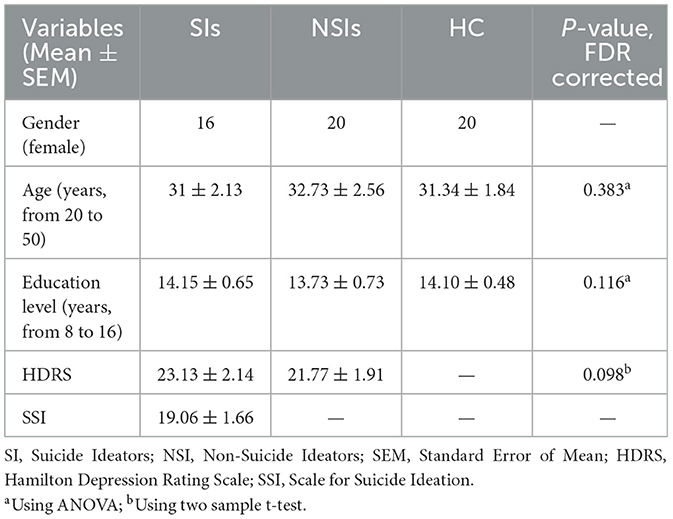
Table 3. Clinical demographics of SIs, NSIs, and HCs.
For each 3D map generated from the fALFF, ReHo, DC, and VMHC analyses, we selected a maximum of seven features [representing different brain regions according to the AAL atlas (Tzourio-Mazoyer et al., 2002)] for classification, based on the guidelines outlined in Al-Zubaidi et al. (2019). We monitored accuracy during training and selected the optimal number of features by setting the maximum to seven. Among the four maps, fALFF resulted in the highest classification accuracy, achieving 92.50% and 87.50% for RFC and EN, respectively. We obtained confusion matrices from the classification results for all four maps and calculated performance metrics. Since we had a classification problem for three groups, the confusion matrix consisted of nine elements (as shown in Table 4). The overall confusion matrix is calculated by averaging the five different confusion matrixes across the folds. Using this matrix, we calculated accuracy, misclassification, sensitivity, recall, specificity, precision, and F1 Score using the following formulas: Accuracy = (TP + TN)/All Predictions, Misclassification = 1 - Accuracy, Sensitivity = Recall = TP/(FN + TP), Specificity = TN/(TN + FP), Precision = TP/(TP + FP), and F1 Score = 2 × (Precision × Sensitivity)/(Precision + Sensitivity). These values are presented in Table 4.
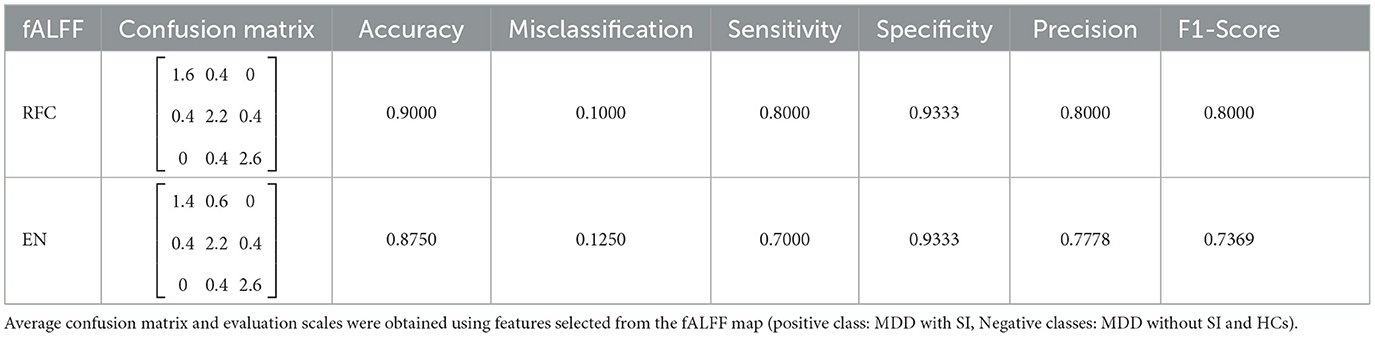
Table 4. RFC and EN classification results.
TP (True Positive): The subject is really SI and we predicted it right. The actual value and predicted value should be the same. So concerning the SI class, the value of Cell 1 is the TP value.
FN (False Negative): The subject is actually SI, but we classified her as MDD or HC. The sum of values of corresponding rows except for the TP value.
FP (False Positive): The subject is not SI, but we consider her as one. The sum of values of the corresponding column except for the TP value.
TN (True Negative): The subject is not SI and we predicted it right. The sum of values of all columns and rows except the values of that class that we are calculating the values for.
TN=(Cell 5+Cell 6+Cell 8+Cell 9)We see that just TP includes one cell, and all other three parameters contain the summation of at least 2 cells. So determining a TP value can be challenging if we not choose or fit our model in the best way.
To have a better understanding of the model and its limitations, there is some details of how we calculate TP, FN, FP, TN in Table 5. When dealing with three classes the confusion matrix is similar to that of two classes, although the calculation is a little different. We considered SI as a reference and compared this group with other groups (MDD without SI and HC).

Table 5. A general example of confusion matrix calculation for a three-category classification problem.
Permutation testing revealed that, only 3 out of 6 selected features fALFF (Frontal_Sup_L, Frontal_Sup_Orb_R, and Cingulum_Mid_R) showed statistically significant differences between individuals with MDD, with and without suicidal ideation. Four brain regions (Frontal_Sup_R, Frontal_Sup_L, Cingulum_Ant_L, and Hippocampus_L) were identified as important for classifying MDDs without suicide and HCs. Five regions (Frontal_Sup_Orb_R, Frontal_Sup_R, Frontal_Sup_L, Cingulum_Mid_R, and Hippocampus_L) were identified as important for classifying MDDs with SI, and HCs.
The above studies and evaluations were also done for the other three connectivity maps. The DC map resulted in 86.00% accuracy for RFC and 87.12% for EN. The ReHo map showed an accuracy of 80.33% for RFC and 76.20% for EN. The VMHC map resulted in 85.60% accuracy for RFC and 85.16% for EN.
The brain regions identified as important features after permutation testing for VMHC, DC and ReHo, respectively were; [Frontal_Sup_L Frontal_Sup_R, Frontal_Sup_Orb_R, Precentral_L] (VMHC), [Frontal_Sup_L, Frontal_Sup_R, Cingulum_Ant_L, Cingulum_Mid_R, Precentral_L] (DC), [Frontal_Sup_L, Frontal_Mid_L] (ReHo) respectively.
Figure 6 illustrates the outcomes of the permutation test performed on the chosen features. Subsequently, after selecting the most significant features, the absolute difference in average values was calculated for each feature separately and labeled as the Ground Truth (GT) score. The vectors of features for both groups underwent permutation 10,000 times to obtain permuted features, and the absolute difference in mean values was computed for each permutation and compared to the GT. If the p < 0.05, it indicates that the majority of absolute differences observed during permutation were smaller than the original GT.
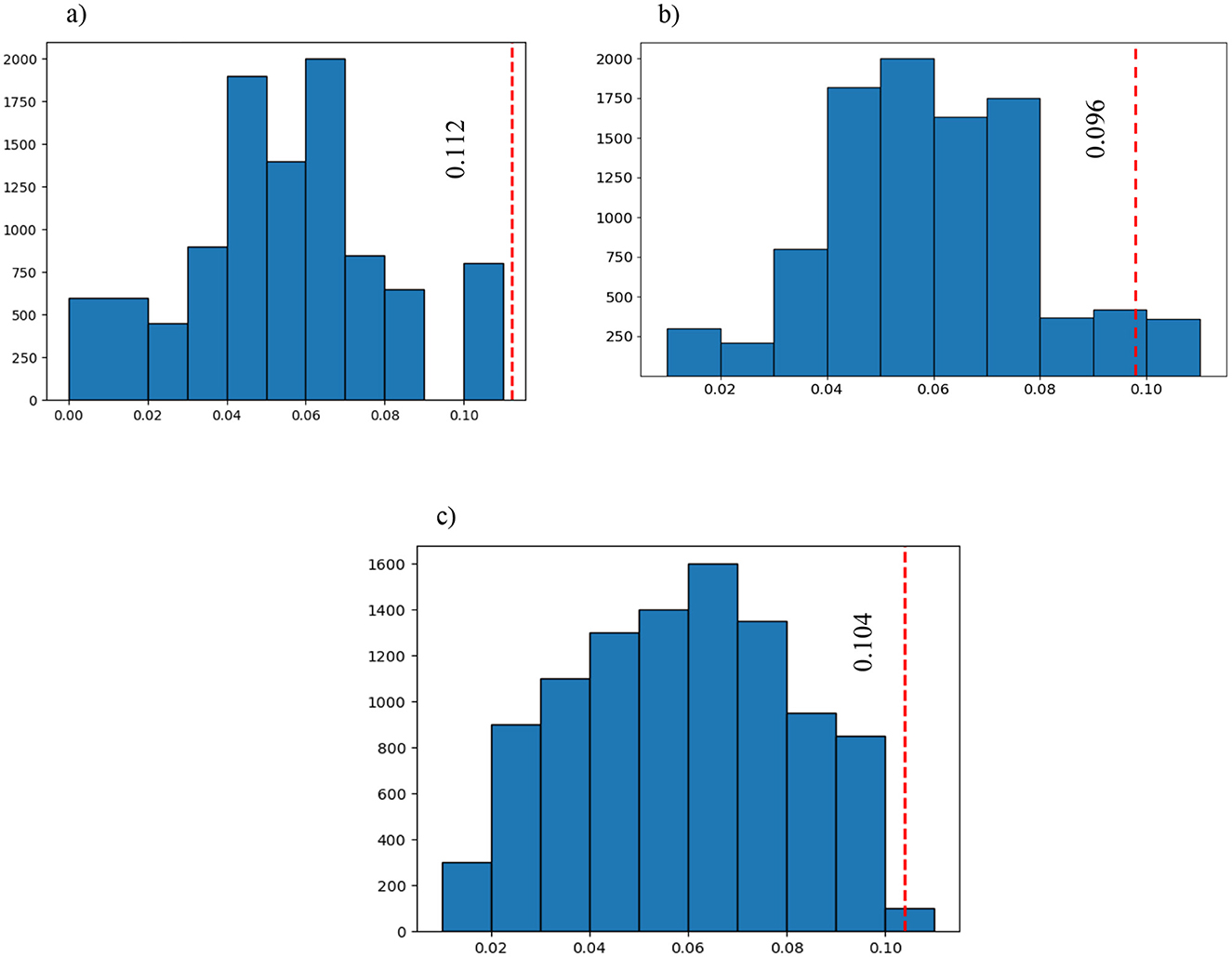
Figure 6. The blue graph represents all the permuted differences for the 3 of the 6 selected features that were significantly different between the three groups (large bin size has been chosen to have a better representation): (A) the first selected feature after SFBS and the permutation test (p = 0.00001); (B) the sixth selected feature after SFBS and the permutation test (p = 0.04239); and (C) the third selected feature after SFBS and the permutation test (p = 0.00241). The red vertical line is the ground truth value which shows the difference between the selected features in the three groups before permutation.
Our research has made a significant discovery in which the brain regions associated with the default mode network (DMN) and central executive network (ECN) were consistently implicated across all connectivity maps. This finding shed light on the critical involvement of these two networks in the development of suicidal ideation in women with MDD. Prompt treatment targeting these networks may help reduce the severity of suicidal thoughts.
To support the results mentioned after the permutation test, we calculated the correlation between SSI scores and mean fALFF values. The fALFF values in Frontal_Sup_L, Frontal_Sup_Orb_R, and Cingulum_Mid_R were negatively correlated with SSI scores (r = −0.675, p = 0.004 for AAL 2, r = −0.608, p = 0.013 for AAL 5, and r = −0.516, p = 0.041 for AAL 33). Figure 7 shows the results of this correlation analysis, which was conducted to investigate the relationship between average fALFF values and SSI scores. In this study, the final stage of comparing classification performance is to generate receiver operating characteristic (ROC) curves for all connectivity maps. An example of this evaluation method can be seen in Figure 8. To evaluate the efficiency of our proposed model against several existing models, we prepared Table 6. Table 6 shows a comparison between different classifiers including RCF and ElasticNet (EN), a Support Vector Machine (SVM), and a simple Convolutional Neural Network (CNN). Results showed that RFC outperformed others, while the CNN-based exhibited the lowest accuracy. This may be attributed to the complexity of CNN and the overfitting of the model caused by an inadequate sample size for the CNN model.
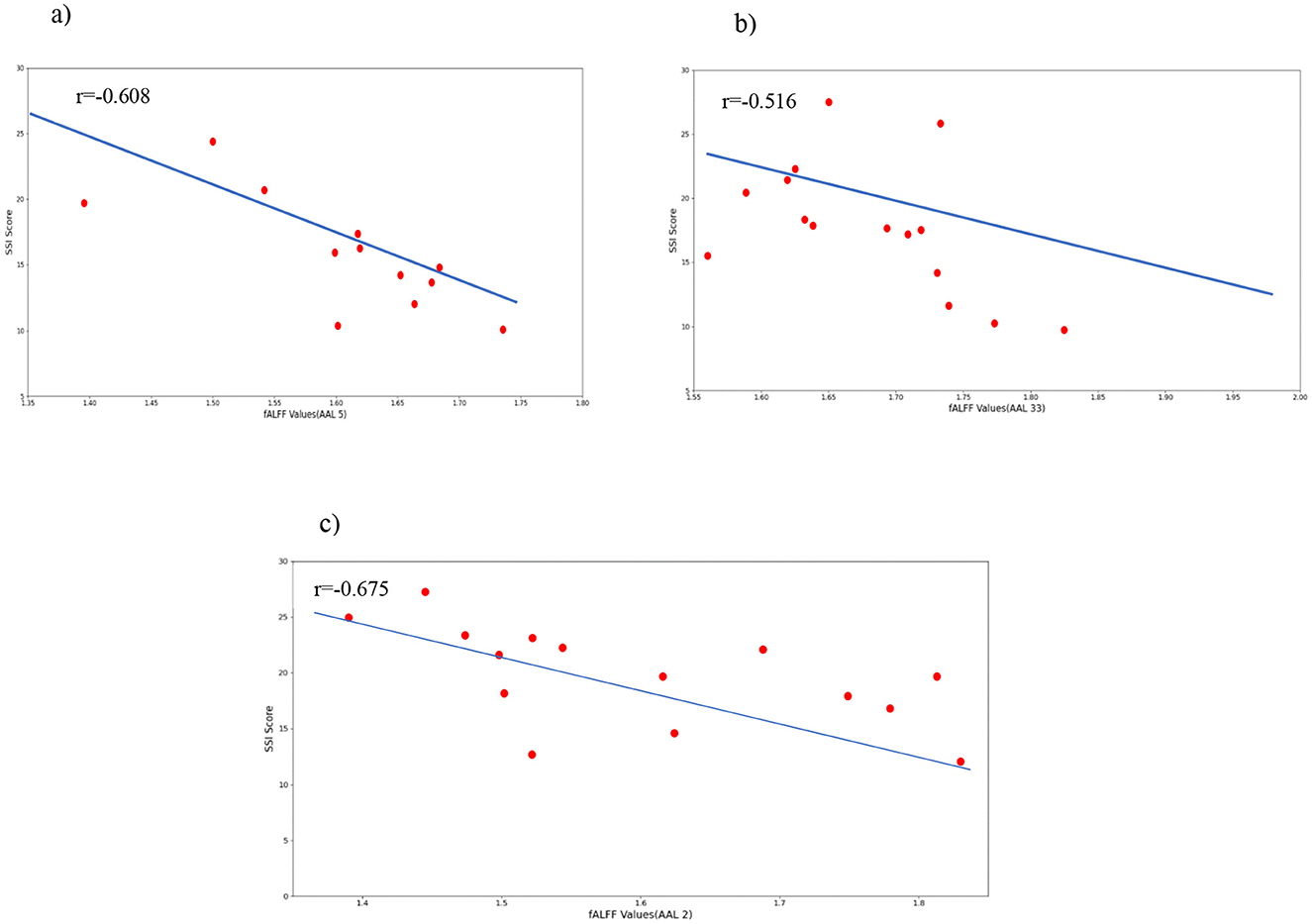
Figure 7. Correlations between selected fALFF values and the clinical behavior scale related to suicide ideation (SSI). (A) correlation between Frontal_Sup_Orb and SSI scores; (B) correlation between Cingulum_Mid and SSI scores; (C) correlation between Frontal_Sup_L and SSI scores.
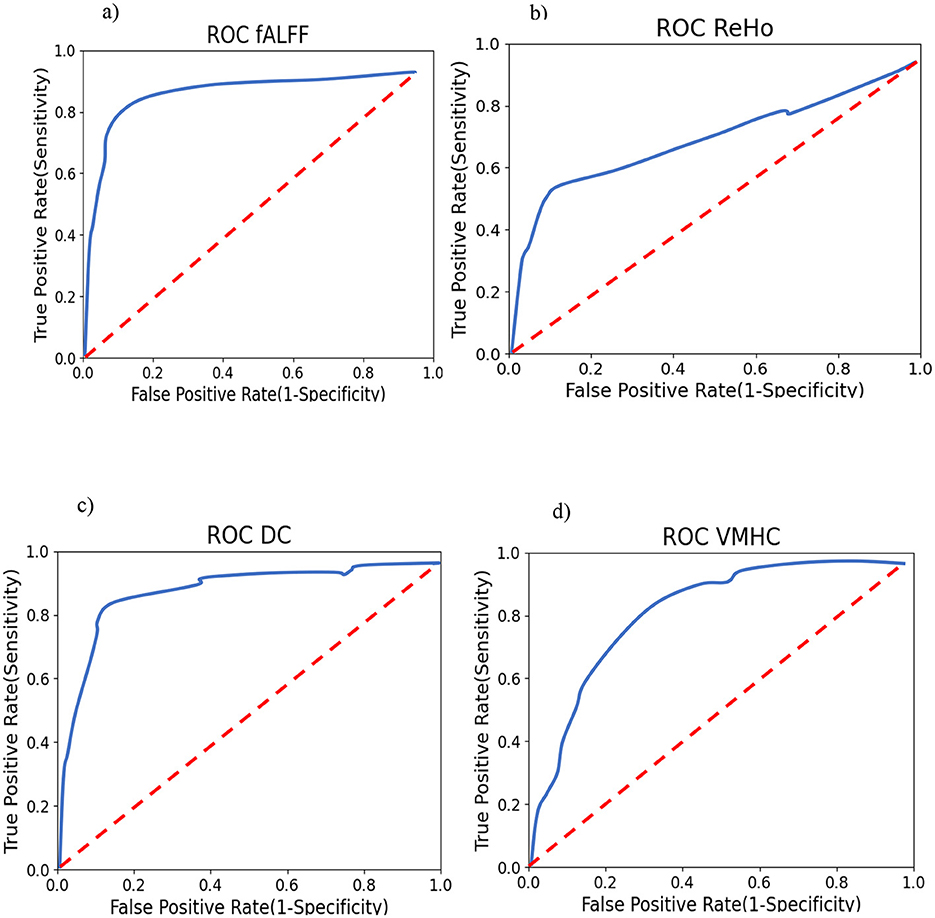
Figure 8. Smoothed One-vs-Rest (suicide ideators vs. rest) ROC curves for RFC. Training (A) using fALFF features; (B) using ReHo features; (C) Using DC features; and (D) using VMHC features.

Table 6. A comparison between the models used in this study and two other methods.
4 DiscussionThis study utilized rs-fMRI to distinguish between MDD female patients with and without clinical suicidal ideation and HCs. The participants in the study exhibited varying degrees of suicidal ideation, ranging from occasional ideation to active planning and determination to carry out an act. Connectivity maps derived from fMRI data were used to classify the groups, employing state-of-the-art feature selection and classification methods. Following feature selection (using SFBS), permutation testing, and RFC as a powerful classifier, significant features of all connectivity maps were identified, including Frontal_Sup and Frontal_Sup_Orb (belong to DMN) and Cingulum_Mid (belong to central ECN), and were determined to be important regions that distinguish between Suicide Ideators (SIs) and non-Suicide Ideators (NSIs). Additionally, activation scores in these regions were negatively correlated with SSI scores, indicating that a reduction in connectivity measures in these nodes may signal an increase in the severity of suicidal ideation and could lead to active suicide attempts. Therefore, prompt treatment targeted at the responsible brain regions is essential to prevent the development of suicidal ideation, which is the primary factor leading to suicide attempts in most MDD patients.
Some studies examined voxel-based connectivity methods examined in this study. A study investigated the ReHo of three groups: MDD patients with treatment-refractory disease (TRD), non-treatment refractory depression, and healthy controls. ReHo was significantly higher in both depressed groups compared to the control group. Furthermore, the TRD group showed additional cerebral regions compared to the non-TRD group (Wu et al., 2011).
Examining the effects of Electroconvulsive Therapy (ECT) on brain function in adolescents with MDD and SI, and the changes induced by ECT as a treatment mechanism for MDD with SI as a hypothesis, significant changes were found in DC values in the inferior frontal gyrus and left hippocampus, showing reductions and increases, respectively (Li et al., 2021). In a study of female MDD patients, fALFF and ALFF were evaluated. Then, depressed and remitted MDD patients were compared to Healthy Controls (HCs). With ALFF values under consideration, a significant difference was found between remitted MDDs and normal controls in the right precuneus. Additionally, with fALFF measurements, marked differences were seen between current MDDs and healthy controls in the right putamen (Jing et al., 2013). Voxel-Mirrored Homotopic Connectivity (VMHC), a more recent method, for calculating inter-hemispheric functional coordination in several regions was used to investigate connectivity templates between two brain hemispheres in drug-free MDD patients and an HC group. Decreases in VMHC values were observed in the right and left posterior cingulate cortex (PCC) (Fan et al., 2018). One critical issue in classification is selecting the best strategy for feature selection. In practical problems involving data representation, many features may be used, but only a few of them are important and relevant to the study's goal (Kira and Rendell, 1992). Most real-world classification problems require supervised learning, where the class probabilities and class-conditional probabilities are uncertain, and each instance is associated with a class label (Dash and Liu, 1997). In feature selection methods such as filter models, the feature selection stage can be independent of the learning process or iteratively assess the value of chosen features based on the learning algorithm's performance, such as in wrapper models. In our study, we utilized wrapper models by selecting features and prompting a classifier for prediction (Tang et al., 1997). Wrapper models use a specific classifier to evaluate the quality of selected features and provide a simple and robust approach to address feature selection, regardless of the learning machine used (Kohavi and John, 1997). By implementing high-order functional connectivity, Sequential forward selection (SFS) in combination with a sparse regression strategy was performed on fMRI data maps to make the classification between mild cognitive impairment patients and normal controls possible with high accuracy of 84.85% (Chen et al., 2017). Sequential backward selection (SBS) deals with a large number of features excellently (Ladha, 2011). According to Wah et al. (2018), after comparing correlation-based and information gain feature selection algorithms as filter approaches and sequential forward and backward elimination as wrapper methods, the wrapper procedures had better performance in selecting appropriate features in both surrogate and real datasets. Furthermore, SFBS had a slightly better function when it came to a small sample size. Random forest is a combination of sequence of tree-based classifiers. RFC and SBS have been utilized for breast cancer detection and prognostic. Compared to other methods like statistical analysis of mammographic features combined with SVM (93.73%), a fuzzy-based data transformation for feature extrication (96.35%), SVM and evolutionary algorithms (97%), this procedure had a higher classification accuracy (99.82%) on Wisconsin breast cancer diagnosis dataset (Nguyen et al., 2013). In Azar et al. (2014), a genetic algorithm was used for feature selection. Then, the features selected from lymph diseases dataset were fed into RFC. This procedure was able to classify the intended data with 92.2% accuracy. In this study, SFBS outperformed SFFS in combination with RFC. According to Masetic and Subasi (2016), RFC was capable of detecting cognitive heart failure with 100% accuracy, better compared to other classifiers like; C4.5 decision tree, k-nearest neighbor, SVM, and artificial neural networks. Six different classifiers including elastic net, RFC, neural network with one hidden layer, SVM, logitboost, and decision tree were compared to observe their power in discriminating twelve different medical datasets. Here, RFC and elastic net had superior performance (Deist et al., 2018). A hypergraph elastic net had the best clustering and classification ability compared to seven other algorithms: G-graph, LE-graph, l1-graph, KNN-hypergraph, semantic correlation hypergraph, sparse subspace clustering, and low rank representation on three different databases (Liu et al., 2016).
As mentioned in the previous studies selecting determinative features is an important part of classification problems on different data types like fMRI, that is why we chose SFBS and Elastic Net penalty as feature selection procedures and utilized RFC and Elastic Net to generate a remarkable power in separating two proposed groups of study. The central executive network (ECN) is responsible for maintaining and controlling information in working memory, decision-making, and problem-solving. It is highly active during cognitively and emotionally demanding tasks and plays a crucial role in emotion regulation during task-oriented processing. Given these functions, it is not surprising that the ECN is involved in major depressive disorder (MDD) and other cognitive disorders (Menon, 2011). In contrast, the default mode network (DMN) shows strong low-frequency fluctuations during passive tasks that require internal mental-state processing, such as remembering, self-referential processing, autobiographical information processing, imagining the future, and thinking about others (Buckner, 2022; Broyd et al., 2009). Dysfunction of the DMN has been linked to rumination and self-preoccupation, which are common symptoms in patients with MDD (Broyd et al., 2009). Differences in functional connectivity values were observed between various networks, including DMN, ECN, and SN, in resting-state fMRI data from MDD patients with suicidal ideation (SI) compared to healthy controls (HCs) (Fattahi et al., 2021). In young MDD patients with and without a history of suicidal behavior, functional connectivity was assessed between the anterior cingulate cortex (ACC) subregions (which belong to the salience network) and other brain areas. Results showed significant differences in subregions of the ACC-superior frontal gyrus between the two groups (Qiu et al., 2020). Another study used voxel-based morphometric analysis to distinguish gray matter volume differences in the prefrontal cortex (PFC), an area associated with the DMN, between individuals with MDD and SI, subjects with MDD but without suicidal thoughts, and normal controls. The study found reduced gray matter volume specifically in the left and right dorsolateral PFC (DLPFC) and right ventrolateral PFC (VLPFC) in the MDD with SI group compared to the HC and MDD without SI groups (Zhang et al., 2020). A study utilizing the sliding-window analysis to calculate the dynamic amplitude of low-frequency fluctuations (dALFF), a proxy for intrinsic brain activity, in individuals with MDD with and without SI as well as normal controls, showed differences in brain dynamics within several regions belonging to the DMN, including the dorsal anterior cingulate cortex (ACG), the left orbital frontal cortex (ORBsup.L), and the left inferior temporal gyrus (ITG.L), as well as the left hippocampus (HIP.L), which is part of the dorsal attention network (Li et al., 2019). Moreover, voxel-wise whole-brain functional connectivity maps were created, and graph-theoretical-based functional connectivity maps were calculated, revealing meaningful differences in functional connectivity strength between suicide attempters and non-attempters in the right orbitofrontal cortex and bilateral dorsomedial prefrontal cortex, both of which belong to the DMN (Chen et al., 2021). Further analyses using network-based statistics and graph-theoretical approaches revealed that MDD patients with suicidal thoughts displayed different correlation values compared to those without SI and normal controls in the superior frontal gyrus (orbital part) and thalamus, suggesting potential issues with decision-making and information integration (Kim et al., 2017).
In a study that investigated MDD without SI, MDD with SI but without SA, and MDD with SA, it was found that widespread functional connectivity attenuation occurred in MDD patients in both the strongly and weakly connected states, involving the intra-network and inter-network connectivity of the primary networks (VIS, AUD, SMN) as well as the high-level cognitive network (DMN) using SVM. The highest accuracy value of this study was 86.84% (Xu et al., 2022).
In another study that perused the MDDs with SA and HCs, showed that compared HCs, adolescent SAs exhibited reduced ALFF values in the bilateral medial superior frontal gyrus (mSFG) and bilateral precuneus which both located at DMN. These decreased ALFF values were negatively correlated with Child Depression Inventory (CDI) scores, while reduced ALFF values in the bilateral precuneus were also negatively correlated with Suicidal Ideation Questionnaire-Junior (SIQ-JR) scores. Support vector machine (SVM) analyses demonstrated diagnostic accuracy rates of 76.8% for reduced ALFF values in the bilateral mSFG and those in the bilateral precuneus (Zhou et al., 2023).
From a neuropsychological perspective, DMN dysfunction is closely related to psychiatric disorders characterized by emotion dysregulation, such as MDD. The brain regions responsible for social regulation, which is considered crucial for emotion processing and regulation, overlap highly with the DMN (Xie et al., 2016). Moreover, the frontoparietal network and the DMN have been found to play an important role in emotion regulation (Pan et al., 2018). A remarkable association between emotion dysregulation and suicidal ideation was found in adolescents of both sexes in the past year. When lifetime suicide attempt was examined as an outcome factor, SI remained the only factor strikingly associated with it. In addition, examination of both prior and post hoc analyzes revealed that limited access to adaptive emotion regulation procedures and the presence of a mood disorder was related to suicidal ideation in the past year (Hatkevich et al., 2019). In another study, affiliation, and emotion regulation approaches, particularly internal dysfunction, showed a strong and moderate association, respectively, with suicidal ideation (Swee et al., 2020). It has also been shown that after applying the Bayesian model to fMRI data, self- and other-referential processing inhibits the flow of information from the left inferior frontal gyrus to some DMN areas in a direct pathway, and this process is consistent with independent inhibition (Soch et al., 2017). The frontoparietal network showed a key function in inhibition, attention, and response control in two experiments based on a go/no-go task (Dodds et al., 2011). On the other hand, cognitive inhibition plays an important role in emotion regulation and adaptation of thoughts and actions (Joormann and Gotlib, 2008). The lack of cognitive inhibition may lead to further suicidal ideation resulting from a lack of regulation of the aroused emotional state and the inspiration of a ruminative and obsessive way of thinking. The suicidal act may be the inevitable consequence of this function in the brain (Richard-Devantoy et al., 2012). In addition, executive dysfunctions such as deficits in cognitive inhibition are common in depressed patients and may be an important factor in suicidality. Indeed, deficits in cognitive inhibition are closely related to suicidal behavior in patients with affective disorders (Richard-Devantoy et al., 2015). Suicidal individuals focus more on negative information, which can be considered an inhibition deficit in these patients. Considering all this, inhibition and emotion regulation, which are important features of risky behavior, are simultaneously linked to DMN and ECN in patients who attempt suicide, in addition to SI.
Machine learning and artificial intelligence (AI) have extended to neurology in recent years. These methods are essential in the creation, management, and preservation of clinical and experimental data. Neuroscience, on the other hand, provides valuable insights into how neural processes occur, which can inform and improve AI algorithms. According to our purpose in the study and the dataset we have, the best method should be selected to get the best results (Mofatteh, 2021; Schuman et al., 2022).
Other populations, like males, people with coexisting conditions, and individuals with cancer, can be future groups of study. Existing brain tumors can certainly be a risk factor for patients with suicide ideation and suicide attempts (Mofatteh, 2021). Damage to the frontal lobe appears to affect divergent thinking, which includes flexibility and problem-solving skills. Additionally, research suggests that attention and memory may continue to be impacted even after significant recovery from a traumatic brain injury or surgery. A notable consequence of frontal lobe damage is a pronounced alteration in social behavior (Jumah and Dossani, 2024; Reber and Tranel, 2019). These are other important matters that need dedicated study in future investigations.
In this study, researchers identified the left superior frontal gyrus (dorsolateral), the right superior frontal gyrus (orbital part), and the right median cingulate and paracingulate gyri as regions with significantly different features extracted from all connectivity measures (ReHo, DC, fALFF, and VMHC). These regions belong to the DMN and the central ECN (frontoparietal network), which have been previously linked to psychiatric disorders characterized by emotion dysregulation such as major depressive disorder (MDD) and suicidal ideation. The study confirms the significant statistical difference between MDDs with and without suicidal ideation and suicide attempters, further emphasizing the importance of these networks in predicting and identifying suicidal ideation.
The study also highlights the reliability of the results as the same regions were found for all measurements and the corresponding features were permuted 10,000 times, demonstrating a consistent and significant difference between the three groups.
It is important to note that this study utilized maps and classification methods to identify regions that can predict suicidal ideation and separate it from non-suicidal ideation, which has not been commonly used in previous studies. Overall, these findings underscore the critical role of the DMN and ECN in understanding and predicting suicidal behavior.
5 LimitationsOne limitation of our study is the small sample size, which may increase type II errors and limit generalizability. To address this limitation, future studies should utilize larger datasets to enhance statistical power. In the current study, this limitation was partially compensated for by a rigorous feature selection process, independent sample validation of the classification model, and augmenting the training dataset. High accuracy was obtained by considering three groups which makes classification more complicated but more generalized.
Another shortcoming of our study is the inability to explore the long-term evolution of suicidality or predict its course. A follow-up study could examine changes in brain connectivity in individuals with suicidal ideation that may precede a suicide attempt. Additionally, investigating the effects of noninvasive clinical treatments, such as transcranial magnetic stimulation (TMS), may provide valuable information for both female individuals with and without suicidal ideation, including those who have attempted suicide. Furthermore, we only studied female MDD patients with suicidal ideation, considering both males and females would be important for generalizing the results. Subsequent studies adopting similar procedures should include both sexes to improve the comprehensiveness of the findings. Another suggestion is to se
留言 (0)