
記住我







Overall, 29 patients with extensive, moderate to severe AD were enrolled and applied ≥ 1 dose of ruxolitinib cream. Patients had a median (range) age of 5.0 (2–11) years, 55.2% were female, 48.3% were White, and 37.9% were Black (Table 1). Mean (SD) affected BSA at baseline was 58.0% (20.0%), with a range of 35.0–92.0% affected BSA at baseline; mean (SD) baseline Itch NRS (as assessed in patients aged 6–11 years) was 8.0 (1.77). Most patients (82.8%; n = 24/29) had used topical treatments in the previous 12 months, the majority of whom (75.0%; n = 18/24) discontinued these due to lack of efficacy (Table 1).
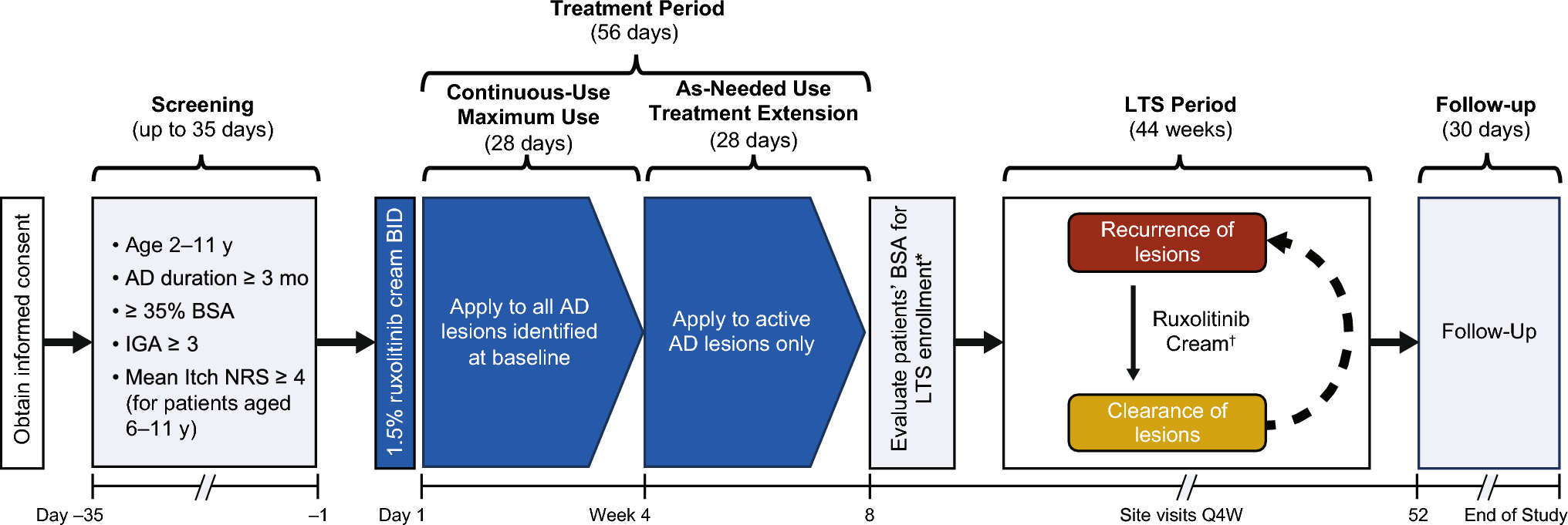
Table 1 Patient demographics and baseline clinical characteristicsOver the 4-week continuous-use, maximum-use period, 96.6% (n = 28/29) of patients completed treatment. In addition, 96.2% (n = 25/26) of patients completed the 4-week treatment-extension period (as-needed treatment of active lesions only), and 63.6% (n = 14/22) of patients completed the 44-week as-needed LTS period. Reasons for treatment discontinuation are shown in Supplementary Fig. 1.
3.2 Safety and TolerabilityDuring the overall study period (i.e., baseline through week 52), treatment-emergent AEs (TEAEs) were reported in 31.0% (n = 9/29) of patients. None were serious, grade 3 or higher, or led to treatment interruption, and none were AEs of special interest (AESI) suggestive of systemic JAK inhibition. No treatment-related TEAEs were reported with long-term, as-needed use. The most common TEAEs during the overall study period included COVID-19, gastroenteritis, influenza, streptococcal pharyngitis, and upper respiratory tract infection (each n = 2; Table 2).
Table 2 Safety summary and tolerability profileOverall, TEAEs were reported in 24.1% (n = 7/29) of patients during the first 8-week treatment period (i.e., continuous use to all baseline lesions with maximal exposure to ruxolitinib cream through week 4, then to active lesions through week 8), and 27.3% (6/22) of patients during the LTS period (i.e., as-needed use). TEAEs reported during the first 8-week treatment period (including the maximum-use period) included COVID-19 (n = 2); folliculitis, nasopharyngitis, arthropod bite, and syncope (each n = 1); and application site folliculitis and application site paresthesia (both in a single patient). Across treatment periods, the incidence of TEAEs was similar regardless of age group (Table 2). One patient had two treatment-related AEs (TRAEs; application site folliculitis and application site paresthesia, both grade 1) during the maximum-use treatment period; both TRAEs resolved without interruption of treatment.
Key hematologic parameters did not change substantially from baseline through week 52 (Fig. 2). Also, no decreases > 1% from baseline in mean serum concentrations of biomarkers of bone formation (BSAP and P1NP) or bone resorption (CTx) were observed through week 8 (data not shown).
Fig. 2
Change in a hemoglobin, b platelets, and c neutrophils from baseline through week 52. IQR, interquartile range; Q1, quartile 1; Q3, quartile 3. IQR is represented by blue/red/green boxes; medians are represented by dark lines; means are represented by O/T/X symbols; outliers are represented by o, x, and + symbols; Q1– (1.5 × IQR) and Q3+ (1.5 × IQR) are represented by whiskers
3.3 PK and Systemic ExposureIn the 26 PK-evaluable patients [mean (SD) affected BSA of 58.9% (20.6%) at baseline for these patients (range 35.0–92.0%); 63.4% (20.2%) in patients aged 2–6 years; 52.9% (20.5%) in patients aged 7–11 years], mean ruxolitinib concentrations and Css during the 4-week maximum-use period were similar across both age groups (Table 3 and Fig. 3). The mean ruxolitinib Css was below the half-maximal concentration of JAK-mediated myelosuppression in adults (i.e., 281 nM [10]), in particular in those with 35–50% affected BSA (Table 3). Two patients with baseline affected BSA ≥ 83% had ruxolitinib Css > 281 nM during the maximum-use period, yet both completed the 52-week treatment period without experiencing any treatment-related TEAEs or any clear decreases in key hematological parameters or bone markers (Table 3 and Fig. 3).
Table 3 Summary of ruxolitinib cream PK parameters and usageFig. 3
Ruxolitinib plasma concentrations through week 4 maximum-use period. Dotted line indicates the half-maximal concentration of STAT3-mediated phosphorylation of thrombopoietin established for adults [10]; 1 patient in the 2–6 years old age group with 83% BSA affected and 1 in the 7–11 years old age group with 92% BSA affected had ruxolitinib plasma concentrations above 281 nM from week 2 (see Table 3 footnotes). IQR, represented by boxes; medians, by dark lines; individual data points are indicated by circles, crosses, and plus signs; Q1– (1.5 × IQR) and Q3+ (1.5 × IQR), by whiskers. *One patient excluded due to outlier concentration. IQR, interquartile range; Q1, quartile 1; Q3, quartile 3; STAT3, signal transducer and activator of transcription 3
Ruxolitinib plasma concentrations were assessed during the 4-week maximum-use period when all lesions were treated with continuous-use 1.5% ruxolitinib cream, with a mean (SD) daily quantity of 8.5 (6.29) g applied. During the 44-week LTS period (as-needed use), plasma concentrations were not collected; however, the mean (SD) daily quantity of 1.5% ruxolitinib cream applied was 3.2 (2.79) g, which was substantially less than that applied during the continuous-use, maximum-use period.
3.4 EfficacyMean affected BSA decreased from 58.0% at baseline (N = 29) to 11.4% at week 4 (n = 26), 10.2% at week 8 (n = 25), and 2.2% at week 52 (n = 14; Fig. 4A). At week 4, only three patients had affected BSA > 20%, of whom two had further improvements in their affected BSA to ≤ 20% at week 8, allowing them to continue into the LTS period. For the third patient, the affected BSA improved from 74% at week 4 to 42% at week 8, resulting in study withdrawal due to lack of efficacy. Additionally, one patient had BSA ≤ 20% at week 4 and > 20% at week 8 (76%), which also led to their study withdrawal (Supplementary Fig. 2). The percentage of patients achieving IGA-TS at weeks 4 and 8 was 53.8% (n = 14/26) and 44.0% (n = 11/25), respectively (Fig. 4B). IGA-TS was generally maintained with as-needed ruxolitinib cream throughout the LTS period, with 53.8% (n = 7/13) of patients achieving IGA-TS at week 52.
Fig. 4
Efficacy of 1.5% ruxolitinib cream through week 52: a mean total percentage affected BSA and b percentage of patients achieving IGA-TS*. BL, baseline; BSA, body surface area; IGA-TS, Investigator’s Global Assessment–treatment success. *IGA-TS defined as an IGA score of 0 or 1 with a ≥ 2-grade improvement from baseline. †Two patients had affected BSA > 20% at week 8 and were ineligible to continue in the LTS period. One patient had affected BSA of > 20% at week 4 (74%) and week 8 (improved to 42%). The other patient had affected BSA ≤ 20% at week 4 and > 20% at week 8 (76%).
EASI-75 responses occurred as early as week 2, with 76.9% (n = 20/26) of patients achieving EASI-75 at week 4 and 84.0% (n = 21/25) at week 8 (Fig. 5); EASI-90 was achieved by 57.7% (n = 15/26) and 52.0% (n = 13/25), respectively. The onset of itch relief in patients aged 6–11 years (n = 13), as measured by reduction in mean Itch NRS, was rapid [week 2: mean (SD; n) change from baseline –5.3 (3.14; n = 10)] and sustained during continuous-use treatment [through week 4: –5.6 (2.89; n = 11)] and treatment of active lesions only [through week 8: –4.9 (0.97; n = 5)]. The percentage of patients achieving NRS4 (averaged over preceding 7 days) increased during the treatment period through week 8 [week 8: 5/5 (100%) evaluable patients achieved NRS4; Fig. 5]. In the 13 patients aged 6–11 years with Itch NRS ≥ 4 at baseline, the median time to achieve Itch NRS4 was 4.0 days (95% CI, 2.0–11.0 days).
Fig. 5
Efficacy of 1.5% ruxolitinib cream during the 8-week treatment period: percentage of patients achieving EASI-75 and EASI-90 and, in children aged 6–11 years, Itch NRS4. EASI-75/90, ≥ 75%/≥ 90% improvement in Eczema Area and Severity Index score from baseline; Itch NRS4, ≥ 4-point improvement in Itch numerical rating scale
During the 44-week (308-day) LTS period (as-needed use), the median (range) number of days off-treatment due to lesion clearance was 93.5 (1.0–279.0) days.
3.5 QoL and PROsChanges from baseline in POEM (children aged 2–11 years), CDLQI (children aged 4–11 years), and IDQoL (children aged 2–3 years) scores indicated substantial improvements in disease severity and QoL, respectively, from as early as week 2, and improvements were sustained through week 52 (Fig. 6).
Fig. 6
Mean (SD) total a POEM (or proxy), b CDLQI* and c IDQoL† scores through 52 weeks of treatment with ruxolitinib cream. BL, baseline; CDLQI, Children’s Dermatology Life Quality Index; IDQoL, Infants’ Dermatitis Quality of Life Index; POEM, Patient-Oriented Eczema Measure. *In patients ≥ 4 years old. †In patients 2–3 years old
In patients aged 5–11 years with baseline PROMIS Sleep Disturbance scores ≥ 14, a clinically meaningful ≥ 6-point improvement was observed in 50.0% (n = 5/10) of patients as early as week 1, increasing to 83.3% (n = 5/6) with longer treatment through week 8, and being maintained through week 52 [85.7% (n = 6/7); Supplementary Fig. 3A]. Also, a clinically meaningful ≥ 6-point improvement in PROMIS Sleep-Related Impairment was achieved by 37.5% (n = 3/8) of patients at week 1, generally improving through week 8 and being maintained through week 52 [85.7% (n = 6/7); Supplementary Fig. 3B].
For patients aged 5–11 years, depressive symptoms as measured by mean (SD) PROMIS PDS T-score improved numerically from 51.4 (10.85) at baseline to 42.5 (8.25) at week 2 and were sustained and further improved through week 52 [37.1 (2.43)]. The effect of AD on family function as measured by mean (SD) DFI score improved numerically from 13.1 (8.66) at baseline to 4.4 (4.85) at week 2 and was sustained and further improved through week 52 to a DFI score reflecting almost no dysfunction [0.7 (1.27)]. For patients aged 4–11 years, health-related QoL as measured by mean (SD) EQ-5D-Y score improved numerically from 71.8 (24.67) at baseline to 93.3 (9.27) at week 2 and was sustained and further improved through week 52 [98.1 (3.02)].
留言 (0)