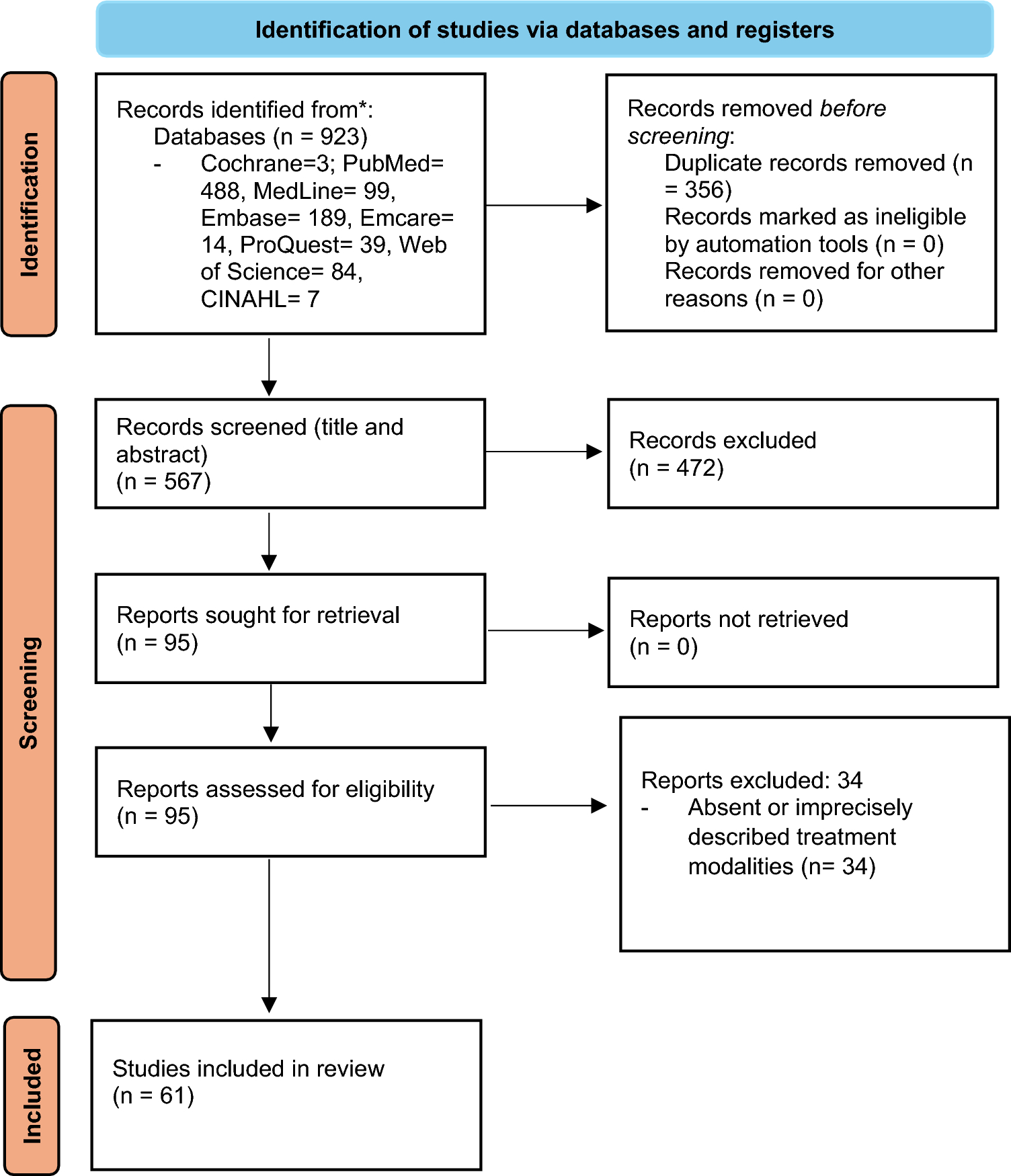
In total, 135 studies were selected for inclusion in this review (Table 2 of the ESM). The evidence for all drugs was generally low and limited to retrospective studies, case reports, and case series. The most robust evidence was available for H1-antihistamines, omalizumab, and various immunomodulators (Table 3, Tables 3–17 of the ESM). Specifically, the review included 23 studies on antihistamines, with most focusing on second-generation H1-antihistamines, and 25 studies on omalizumab, reflecting its growing role in UV management. Systemic glucocorticosteroids stood out as a treatment with multiple single-treatment studies featuring larger patient cohorts. Other drugs, such as dapsone (13 studies) and anti-CD20 antibody rituximab (ten studies), were also well represented, highlighting their importance in managing more severe and refractory cases.
Table 3 Summary of the use of major drugs for systemic therapy in UV3.1 Second-Generation H1-Antihistamines
Overall, 141 patients with UV (77 of whom had NUV) from 23 publications received different second-generation anti-histamines (sgAHs) at a standard dose or up-titrated up to four times the standard dose (n = 5). Two patients received concomitant ranitidine (an H2-antihistamine), whereas eight patients received an additional first-generation H1-antihistamine (hydroxyzine, up to 50 mg/day). The duration of treatment varied from 10 days to 8 years. Resolution of skin lesions with the isolated use of sgAHs occurred in 3.5% of patients (n = 5/141), and skin lesions improved in 6.4% (n = 9/141) of patients with concomitant use of oral prednisolone or colchicine. SgAHs, used at standard or higher than the standard dose, failed to effectively improve skin lesions in the remaining 90.1% patients (n = 128/141). These patients commonly switched to the use of SGC, immunomodulators, or omalizumab for their UV. SgAHs have not been reported to have any effect on extracutaneous symptoms, and no treatment-emergent adverse events (AEs) were reported (Table 3 of the ESM).
In line with our recent systematic review, we found that sgAHs are of limited efficacy in UV [2]. However, given their safety profile, sgAHs can be tried in patients with UV with mild symptoms and pruritus, those who have signs of a CSU/UV overlap, and possibly also in patients with more severe disease as an adjunct therapy, along with systemic immunomodulators or biologics. SgAHs are generally safe, even as a long-term treatment; however, some AEs are possible, such as tiredness and somnolence, especially at high doses [11]. Elderly patients, especially those with renal, hepatic and/or cardiac disorders may be at risk while taking high doses of some sgAHs. Cetirizine and loratadine are considered to be safe in pregnant and breastfeeding women [12, 13].
3.2 Monoclonal Antibodies
Among biologic therapies, the most substantial evidence for treating UV is available for omalizumab, a humanized recombinant anti-immunoglobulin E (IgE) monoclonal antibody, and rituximab, a monoclonal antibody targeting the B-lymphocyte antigen CD20. Additionally, there is evidence for the use of canakinumab, an interleukin (IL)-1β antagonist, and anakinra, an IL-1-receptor antagonist.
3.2.1 Omalizumab (Anti-IgE)
Between 2009 and 2023, omalizumab was administered to 108 patients with UV, primarily those with NUV (n = 52/108), across 25 studies, most of which were case reports (Table 4 of the ESM). Cutaneous symptoms improved in 76% of patients (n = 82/108), many of whom achieved full clinical remission. Extracutaneous symptoms, such as arthralgia or abdominal pain, improved in 40% of patients (n = 10/25). Non-serious AEs, including fever and laboratory abnormalities, were reported in 12 patients during or after the treatment.
Omalizumab is approved for the treatment of sgAH-refractory CSU as the second-line therapy, administered at a dose of 300 mg by subcutaneous injection every 4 weeks in adults and adolescents 12 years of age or older [14]. Dosing in CSU is independent of the serum IgE level or body weight, although low and high levels of total IgE have been described as a marker of slow/non-response and fast/good response to omalizumab, respectively [15]. In studies of urticaria and asthma, omalizumab was well tolerated, even with long-term use [16, 17]. It is also considered safe in pregnancy, in younger children, and in elderly individuals, although it is not licensed for these subpopulations of patients with CSU [18].
3.2.2 Canakinumab and Anakinra (Anti-IL-1)
Krause et al. used a single dose of canakinumab (300 mg subcutaneously) in an open-label study in ten patients with UV (9 NUV and 1 HUV). Cutaneous and systemic symptoms, as well as laboratory markers of inflammation, improved within 15 days in 70% of patients (n = 7/10), followed by relapse in one patient after 4 weeks [4]. In a French multicenter study, six patients with UV (two NUV and four HUV) with associated skin, gastrointestinal, and articular symptoms were treated with anakinra (with one case later switching to canakinumab). Five patients experienced a complete remission and one showed a partial improvement of cutaneous and systemic symptoms, but at least four relapsed upon drug discontinuation [19]. In a case report of NUV, presenting for more than 3 years with wheals, fever, and elevated C-reactive protein, the patient responded to anakinra, further supporting the potential of IL-1 inhibition in UV [20] (Table 5 of the ESM).
3.2.3 Rituximab (Anti-CD20)
In two larger case series, rituximab, an anti-CD20 therapy, demonstrated a complete and fast resolution of skin and systemic symptoms, as well as laboratory parameters in 71% of patients (n = 10/14) who had previously not responded to treatment with SGC and other conventional immunosuppressants [21, 22]. In every one of the reviewed publications, all patients treated with rituximab (n = 21) showed improvements in their skin symptoms (Table 6 of the ESM). All patients with systemic involvement who received rituximab also showed improvement in those symptoms (n = 20), including those affecting the kidneys, joints, lungs, eyes, and gastrointestinal tract. Although serious adverse reactions to rituximab, including allergic reactions and severe cytopenia, have been reported in the literature [23], none of the publications reviewed in this study reported any AEs following rituximab therapy.
In summary, omalizumab can be used as an off-label treatment for UV, especially in patients with NUV and those with mild disease, presenting with CSU-like symptoms, including itchy wheals, and minimal or no fever, arthralgia, abdominal pain, or other systemic symptoms. Similar to CSU treatment, omalizumab at higher doses, shorter intervals, or both can be considered in patients with UV with an insufficient response to the licensed dose within 3–6 months [24]. Anti-IL-1 and anti-CD20 therapies can be considered in refractory UV cases but their use is limited by high costs and available evidence.
3.3 Immunomodulators3.3.1 Systemic Glucocorticosteroids
Systemic glucocorticosteroids are potent anti-inflammatory drugs frequently used to manage various inflammatory dermatologic conditions, including UV. They work by suppressing inflammation and modulating immune responses, thereby alleviating symptoms and improving patient outcomes. In seven studies involving 287 patients with UV treated with SGC from 2007 to 2023, a common dosage regimen was 0.5–1 mg/kg per day (Table 7 of the ESM). Treatment typically began with daily administration for 1–2 weeks, followed by gradual tapering of the dosage. Significant improvements in skin symptoms were observed across all studies that ranged from 44.8% (n = 39/87 [3]) to 100% (n = 20 [25]) of patients. Likewise, improvement in extracutaneous symptoms was noted in 32% (n = 57 [21]) to 93.3% (n = 56/60 [5]) of cases. These findings underscore their role as a cornerstone in the therapeutic armamentarium for this condition. However, because of potential side effects such as hyperglycemia, arterial hypertension, adrenal suppression, and osteoporosis, long-term use of SGCs should be avoided [26].
3.3.1.1 Combined Immunosuppressive Treatment
Other immunosuppressive medications were used in several patients with difficult-to-treat UV including those with underlying conditions such as SLE, often in combination with SGC. Cyclosporine A, methotrexate, azathioprine, cyclophosphamide, and mycophenolate mofetil (MMF) are typically employed as second-line therapies for moderate-to-severe cutaneous vasculitis [27, 28]. The combined use of SGC and immunosuppressants has been shown to improve efficacy in controlling both cutaneous and extracutaneous manifestations of UV compared with SGC alone, although response rates and treatment duration may vary among different agents [28]. One study reported response rates of 74% for cutaneous symptoms and 63% for immunologic responses, defined as normalization of C3 and/or C4 levels, in cases of refractory and/or relapsing disease when SGCs are combined with conventional immunosuppressive agents [21]. Furthermore, supplementary immunosuppressive therapy has been beneficial in reducing SGC dosages.
3.3.2 Cyclosporine A
In three case reports, female patients with UV received oral cyclosporine A in daily doses that ranged from 2.5 to 5.0 mg/kg (Table 8 of the ESM). The treatment improved urticarial lesions in all cases (n = 3/3), and alleviated arthralgias in one case. In a meta-analysis and systematic review of CSU studies, cyclosporine A was effective in 54–73% of patients at doses of 1–5 mg/kg/day [29]. These findings suggest that cyclosporine A is a viable treatment option, particularly for managing the skin symptoms of UV.
3.3.3 Methotrexate
In three studies including 15 patients, methotrexate at doses of 5–20 mg weekly was effective in achieving skin remission (n = 13/15) and long-lasting complete disease remission as well as reducing the SGC dose [27, 28] (Table 9 of the ESM). Methotrexate is generally reported to be a well-tolerated medication; [30, 31] however, paradoxical exacerbation of UV symptoms [27, 32], fatigue, hair thinning, hepatotoxicity, myelosuppression with pancytopenia, and gastrointestinal symptoms is possible[2].
3.3.4 Azathioprine
Azathioprine was used in refractory UV cases with doses adjusted based on thiopurine methyltransferase levels. Azathioprine allowed a SGC dosage reduction and resolution of cutaneous lesions [27, 33, 34] (Table 10 of the ESM). Two case reports suggested possible benefits in resolving lung and kidney impairment, respectively [33, 35]. In a larger case series of 18 patients, azathioprine improved cutaneous and extracutaneous symptoms in 83% (n = 15) and 72% (n = 13) of patients, respectively [22]. Adverse effects such as dose-dependent leukopenia, hepatotoxicity, and nephritis underscore the need for vigilant patient monitoring [36,37,38]. In one reviewed case (n = 1/21), azathioprine was discontinued because of an increase in hepatic cytolysis parameters [37].
3.3.5 Cyclophosphamide
In case reports of patients with UV aged between 12 and 65 years (58% female, n = 12) [Table 11 of the ESM], cyclophosphamide reduced skin symptoms in 58% of patients (n = 7/12) and improved extracutaneous symptoms, such as glomerulonephritis [39], in nearly all patients (n = 11/12). Cyclophosphamide is often used in combination with SGC to enhance efficacy and mitigate the severity of side effects. While only one study reviewed reported non-serious AEs in two patients [40], cyclophosphamide can have potentially severe side effects including myelosuppression, bladder and gonadal toxicity, and cytopenia [41]. These risks highlight the importance of careful patient selection, vigilant monitoring, and a thorough assessment of the risk-benefit ratio.
3.3.6 Mycophenolate Mofetil (MMF)
In the studies reviewed, MMF improved cutaneous symptoms in 75% of patients (n = 9/12), including a larger study of ten patients where 70% benefited [21] (Table 12 of the ESM). Mycophenolate mofetil also demonstrated positive effects on extracutaneous manifestations of UV in two case reports. Although it has a favorable safety profile with no reported AEs in the studies reviewed, MMF was most commonly used as a fourth-line therapy [21]. Nevertheless, it remains a viable therapeutic option for patients with refractory or severe cases of UV [42]. In addition, MMF has been proposed as maintenance therapy after cyclophosphamide and dexamethasone pulse in patients with UV [43].
3.3.7 Dapsone
Several publications (Table 13 of the ESM) reported the use of dapsone in UV, mainly in HUV, most frequently at a dose of 100 mg daily (range: 25–150 mg daily). Dapsone has been shown to be effective for cutaneous symptoms in almost all cases, including the resolution of wheals, burning, and pain. Dapsone has also been shown to improve musculoskeletal pain, fever, fatigue, and gastrointestinal symptoms. In three of 11 case reports, dapsone therapy was discontinued because of serious side effects, including severe drug reactions, after just a few weeks of use [44,45,46]. However, this was typically observed at a dose of 100 mg or more. In addition, dapsone was often used in combination with other systemic therapies, making it difficult to assess its independent effectiveness.
3.3.8 Hydroxychloroquine (HCQ)
In several publications (Table 14 of the ESM), hydroxychloroquine (HCQ) reportedly helped approximately 57% of patients with UV (n = 74/130). Daily dosages ranged from 100 to 400 mg, with 400 mg/day being the preferred dosage [2]. In two larger case series as well as a web-based questionnaire of patients with UV, response rates of 75% (n = 18/24 [22]), 54% (n = 14/26 [47]), and 76% (n = 36/47 [3]), respectively, were reported. HCQ was frequently administered alongside SGCs. Combining HCQ with prednisolone (0.5 mg/kg/day) achieved complete remission in 88% (n = 15/17) of HUV cases, with the authors typically initiating treatment with both drugs and then continuing with HCQ alone to mitigate the long-term adverse effects of SGCs [2, 48,49,50]. One study indicated that HCQ was as effective as SGCs while exhibiting a favorable AE profile [22]. The efficacy of HCQ typically became apparent within 3 months of treatment initiation. It was predominantly used for treating HUV/hypocomplementemic urticarial vasculitis syndrome (HUVS), leading to complete remission of skin symptoms and improvements in extracutaneous symptoms affecting the joints, lungs, and eyes. Additionally, HCQ contributed to improved immunological markers among patients with UV, including increased complement components [2].
3.3.9 Intravenous Immunoglobulins (IVIg)
Intravenous immunoglobulins (IVIg) exhibit immunomodulatory and anti-inflammatory properties and have been effectively utilized in several cutaneous autoimmune diseases including SLE, dermatomyositis, pemphigus, and chronic urticaria [51]. However, the strength of evidence supporting the use of IVIgs in treating UV is limited. IVIgs were effective at doses of 1–2 g/kg administered every 4 weeks in four case reports involving patients with UV aged between 4 and 76 years. This cohort included two patients with HUV and one patient with HUVS, all of whom achieved full clinical remission (Table 15 of the ESM).
In summary, SGC should be considered in moderate-to-severe cases of UV with pronounced systemic manifestations. However, long-term use should be avoided, particularly in vulnerable patient populations, such as older patients with comorbidities. The dosage should be tapered as soon as possible to mitigate long-term adverse effects, though this may not always be possible, especially in refractory UV cases. Other immunomodulatory or immunosuppressive therapies may serve as SGC-sparing agents and can be beneficial for patients with UV with multi-organ involvement and underlying rheumatic diseases, such as SLE. Nonetheless, similarly to SGCs, these therapies can have potentially severe side effects, necessitating a careful evaluation of the risk–benefit ratio and close monitoring of both clinical and laboratory parameters.
3.4 Other Treatments
Non-steroidal anti-inflammatory drugs were used for the treatment of UV in numerous studies (Table 16 of the ESM). Several different agents and dose regimens, often combined with additional drugs, are described in the literature with inconsistent effects on cutaneous and extracutaneous symptoms. Importantly, most reports are single case reports or small case series, and no controlled studies are available, rendering it difficult to assess the benefits of non-steroidal anti-inflammatory drugs in the treatment of UV. We suggest that non-steroidal anti-inflammatory drugs can be taken as needed or continuously as supplementary therapy by patients with UV with skin pain and pain of other localizations, such as abdominal pain and/or fever.
In three studies reporting on colchicine as a UV treatment, 30% of patients (n = 20/66) benefited from the therapy (Table 17 of the ESM). Both patients with NUV/HUV were treated with doses that ranged between 0.5 mg/day and 0.6 mg three times a day (1.0–1.2 mg/day in most cases), resulting in complete remission of skin symptoms and improvements in extracutaneous symptoms affecting the joints and gastrointestinal system in some cases [2]. In small case series and case reports, colchicine was found to be effective in only around 16% of patients [2, 52], and the response rate in one of our studies was also low [3]. The efficacy seems to increase when colchicine is combined with SGC, and 92% (n = 13) of patients responded to the combined treatment [2, 53]. However, the efficacy in these studies may be associated with the effectiveness of SGC. Reports on the efficacy of H2-antihistamines (no data), anti-tumor necrosis factor-α antibodies (no data), anti-IL-6 receptor (tocilizumab), montelukast, tranexamic acid, doxepin, thalidomide, pentoxifylline, plasmapheresis, and danazol (Table 18 of the ESM) are largely limited to individual case reports, and in most of them, the drugs showed very limited or no benefit, or the efficacy was not clear as they were often administered in combination with other medications [30, 44, 48, 54,55,56,57,58,59,60,61,62,63,








留言 (0)