
記住我



This study followed the guidelines of the Institutional Animal Care and Use Committee (IACUC) and obtained approval for the animal procedures before commencement. Sterile surgical techniques were required, as referenced in the Guide for the Care and Use of Laboratory Animals and the Federal Animal Welfare Regulations. The study was approved by the Institutional Animal Care and Use Committee of Dalian Medical University (No.AEE23058). Twelve-week-old nulliparous female Wistar rats were acquired (n = 21). After prolapse modeling [21], the prolapsed rats (n = 18) were housed in an animal room with standard humidity (45−50%), temperature (22 ± 2)°C, and a 12-h light cycle (12 h daylight/12 h dark), with free access to food and water.
MeshThree prolapse meshes were used: PP mesh (n = 6), PCL scaffolds (n = 6), and decellularized porcine (SIS) scaffolds (n = 6). PP mesh is non-absorbable, whereas PCL and SIS scaffolds are absorbable. Before the UPS, the three meshes were soaked in 75% alcohol for 30 min, rinsed with PBS three times (each rinse lasting 1 min), and then exposed to UV light for 30 min. Uniaxial tensile testing was conducted on the three meshes, each cut into rectangular pieces measuring 20 mm in length and 2 mm in width.
The Procedure of Unilateral Presacral SuspensionProlapsed Rat ModelBased on our previously developed prolapsed rat model [21], a special vacuum suction device suitable for the rat's vagina was completely inserted into the rat's vagina. The rat's cervix and part of the fornix tissue were pulled outside the vaginal opening by negative pressure. The traction criterion was that the cervix was pulled 5 mm from the external vaginal introitus. The cervix was sutured with 3–0 Prolene sutures in a cross pattern, leaving a 2-cm-long thread for subsequent traction. Traction was performed nine times daily, each time for 2 min, with a 1-min rest interval, for 7 days. Then there were 7 days of recovery before UPS. The prolapsed cervix was exposed outside the introitus with sutures from the prolapse modeling left in place to facilitate the evaluation of postoperative prolapse repair (Fig. 1A).
Fig. 1
The procedure of unilateral presacral suspension (UPS). A The cervix of the prolapsed rat is exposed at the vaginal opening, with sutures from the prolapse modeling left in place to facilitate the evaluation of postoperative prolapse repair. B Exposing the abdominal cavity. C The anatomical relationship of the uterine artery (UA), the vesical artery (VA), the superior vesical artery (SVA) and the ureter (Ur). D Dissecting the bicornuate uterus and ovaries. E Subtotal hysterectomy. F Pelvic anatomy of the rat after removal of the posterior peritoneum and part of the presacral muscle group. The yellow dotted area indicates a strong prevertebral ligament, which is the site for mesh fixation. 1 First and second sacral vertebrae space; 2 abdominal aorta; 3 sixth lumbar nerve; 4 pudendal nerve; 5 common iliac artery; 6 sacrococcygeus ventralis medialis. G Confirming the fixation site (yellow dotted area). H Using angled forceps to create a mesh tunnel. I The status of mesh fixation and posterior peritoneum closed. The white dotted area indicates the position of the mesh.Ov ovary, Ut uterus, BL bladder
Anesthesia and DisinfectionBefore anesthesia, the rats were fasted for 12 h to minimize the impact of intestinal contents during surgery. Pentobarbital sodium (50 mg/kg) was administered via intraperitoneal injection to anesthetize the rats. After anesthesia, streptomycin (28 mg/kg) was injected into the inner thigh to prevent infection. The anesthetized rats were then placed on a constant temperature heating pad. The abdominal hair was removed, and the vagina and cervix were disinfected with iodophor.
Exposing the Abdominal CavityThe abdominal hair was removed. After disinfection and draping, a 30-mm longitudinal incision was made along the midline of the abdomen, 15 mm above the urethral opening. The muscle groups were then separated, and a retractor was used to expose the abdominal cavity (Fig. 1B).
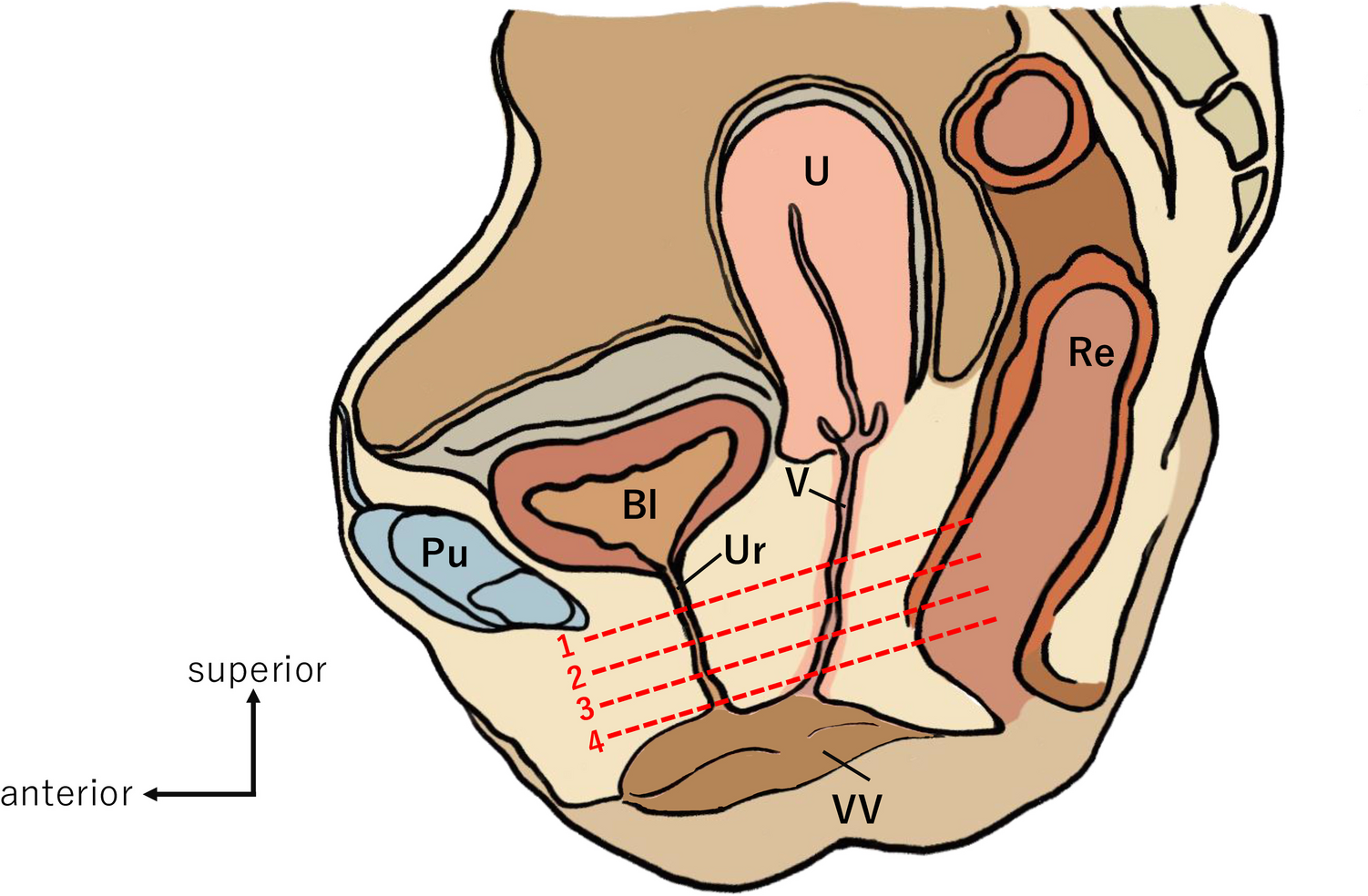
Ligation of the Bilateral Uterine ArteriesThe superior vesical artery originates from the internal iliac artery, branching cranially to form the uterine artery and caudally to form the vesical artery [28]. Simultaneously, the lower segment of the ureter passes through the bifurcation of the superior vesical artery, entering the bladder along the outside of the vesical artery. Therefore, when ligating the uterine artery, it is crucial to avoid ligating other important blood vessels or the ureter (Fig. 1C).
Dissecting the Bicornuate Uterus and OvariesAfter ligating the uterine arteries on both sides, the ovaries and uterus could be freed. By grasping the lower edge of the ovary and the ovarian uterine artery, the electrocautery hemostasis pen was applied along the lower edge of the angled forceps to free the ovaries and uterus (Fig. 1D).
Subtotal HysterectomyThe uterus was cut at the upper edge of the cervix, and the cervical stump was sutured with 8-0 non-absorbable silk. One end of the mesh was then fixed to the dorsal side of the cervical stump with 8-0 non-absorbable silk (Fig. 1E). Preserving the cervix allowed for the retention of the 3-0 Prolene sutures on the cervix, facilitating postoperative observation of the cervical suspension status.
Confirming the Anterior Vertebral LigamentsFigure 1F illustrates the rat pelvic structure post-euthanasia, following the separation of the pelvic floor muscles. The space between the first and second sacral vertebrae is located to the right of the confluence of the abdominal aorta and the common iliac artery. The anterior vertebral ligaments, which are exposed, are robust enough to endure the force of cervical suspension.
Mesh Tunnel and FixationThe retroperitoneum was opened to the right of the confluence of the abdominal aorta and the common iliac artery, exposing the anterior vertebral ligaments (Fig. 1G). Angled forceps were inserted into the retroperitoneum and exited below the cervical stump. These forceps grasped the other end of the mesh, positioning it entirely beneath the posterior peritoneum (Fig. 1H). The mesh was then pulled upward and secured to the anterior vertebral ligaments using 8-0 non-absorbable silk. To prevent the mesh from being exposed to the abdominal cavity and eroding organs such as the bladder and intestines, the posterior peritoneum was sutured (Fig. 1I). The abdominal cavity was closed, the skin was sutured and disinfected, and the rats were transferred to a constant temperature box for 24-h observation.
Specimen Collection and PreservationThe parametrial fascia (PMF) and the USLs were collected from normal rats (n = 3). The uterus and its surrounding supportive tissues were completely removed and laid flat on the operating table. A horizontal incision was made along the upper edge of the cervix. The part connected to the uterine body was identified as the PMF, and the part connected to the cervix was identified as the USL (Fig. 2A, B) [22]. Four weeks after the UPS, the mesh complexes were collected from the prolapsed rats (n = 18; Fig. 2C, D).
Fig. 2
Biomechanical testing. A The intact uterus and its surrounding supporting tissues are flattened on the tray. The horizontal dashed line indicates the cut along the upper border of the cervix. The vertical dashed line indicates the cut along the midline of the cervix. B Four parts after cutting, right parametrial fascia (RPMF), left parametrial fascia (LPMF), right uterosacral ligament (RUSL), and left uterosacral ligament (LUSL). C Pelvic anatomy observed after opening the abdominal cavity. D Ligament-like structure 4 weeks after unilateral presacral suspension. E The PMF is secured on a mechanical testing machine. RPMF right parametrial fascia, LPMF left parametrial fascia, RUSL, right uterosacral ligament LUSL left uterosacral ligament
Mechanical TestingThe specimens tested on the uniaxial testing machine included three different meshes (PCL, SIS, and PP), PMF, USL, and mesh complexes (PCL complex, SIS complex, and PP complex). PMF and USL served as controls to compare the strength of the mesh complexes 4 weeks after UPS. Each specimen was mounted on the mechanical testing machine (Fig. 2E). Before each test, the specimen was preloaded to 0.05 N and then preconditioned for ten cycles at an extension rate of 25 mm/min within an elongation range of 0 to 2 mm, corresponding to cycling in the elastic region of the load-elongation curve. After preconditioning, a uniaxial failure test was immediately performed at the same extension rate. The load-elongation curve and failure mode were recorded from data points collected every 0.02 s using the provided software, then imported into Excel for analysis. The ultimate load (N) at failure was defined as the highest load before the failure of the target mesh tissue.
Masson’s Trichrome Staining and Collagen Ratio AnalysisMasson’s trichrome staining was performed according to the manufacturer’s instructions. The slices were then observed and photographed using an optical microscope. Using the image-processing software ImageJ, four square areas around the mesh were randomly selected from the mesh complex slices, whereas the parts close to the cervix were selected from the USL slices. Both were analyzed on 10 × pathology slides to measure the collagen ratio.
Statistical AnalysisStatistical analyses and graphical representations were performed using GraphPad Prism 9 (GraphPad Software, USA). Data are presented as mean ± standard deviation. A two-tailed Student’s t test was used to assess differences between the two groups. Differences among groups in ultimate load and collagen ratio were evaluated using a one-way analysis of variance. Statistical significance was defined as (p < 0.05).
留言 (0)