
記住我



This randomized, controlled, single-blind, multicenter, parallel group trial was performed to compare the efficacy and safety of an electronic bidet with a lower-force fountain-type water flow system for anal pain control and wound cleansing after hemorrhoidectomy with those of the conventional warm sitz bath. Patients who required hemorrhoidectomy were eligible for inclusion in this study. The inclusion criteria were adult patients aged 19–70 years who needed hemorrhoidectomy because of hemorrhoid bleeding or protrusion. Exclusion criteria included a history of previous anal surgery, anal abscess or fistula, Crohn’s disease, pregnancy or breast feeding, history of treatment for malignancy within 5 years, immunosuppressant or steroid use, human immunodeficiency virus infection, drug allergy, or any uncontrolled medical problems. All included patients provided written informed consent. The study was conducted in compliance with the Declaration of Helsinki and approved by the institutional review board (IRB) of Seoul National University Hospital (1412-080-633). The trial is registered on ClinicalTrials.gov (NCT02353156, date: 02/02/2015).
Randomization and maskingThe patients were randomly assigned 1:1 before hemorrhoidectomy to either the electronic bidet or sitz bath (control group) for anal pain control and wound cleansing after hemorrhoidectomy using a block permutation approach. The block size was 4 or 6. Random numbers were computer generated by SAS 9.4 (SAS Institute, Cary, NC, USA). Allocation was performed through the Interactive Web Randomization System (IWRS) of the Medical Research Collaborating Center (MRCC) of Seoul National University Hospital by a researcher who was independent from the progress of the study. Throughout the entire study period, the surgeon remained blinded to the treatment the participants received.
ProceduresConventional closed or semiclosed hemorrhoidectomy was performed for all patients, and seven surgeons from four hospitals participated in this study. The anoderm and mucosa around the hemorrhoid pile were incised, and careful dissection between the submucosa and internal sphincter muscle was performed with meticulous hemostasis. The main protruding piles were removed completely. The hemorrhoidal artery and pedicle were sutured, and the wound was closed with absorbable suture materials. Preoperative mechanical bowel preparation was recommended 1 day before the operation, and perioperative antibiotics were used immediately before the operation and 1 day after the operation. The patients resumed an oral diet 1 day after the operation. Thirty milligrams of ketorolac tromethamine, a nonsteroidal anti-inflammatory drug (NSAID), was administered by intravenous injection on the operation day and 1 or 2 days after the operation during hospitalization to relieve postoperative anal pain. Intravenous injections could be administered 3 times a day for a total amount of no more than 90 mg. After discharge from the hospital, the patients could take 10 mg ketorolac tromethamine tablets tid or qid orally for 6 days after the operation. The total amount of oral medication used was determined at 1 week after the operation.
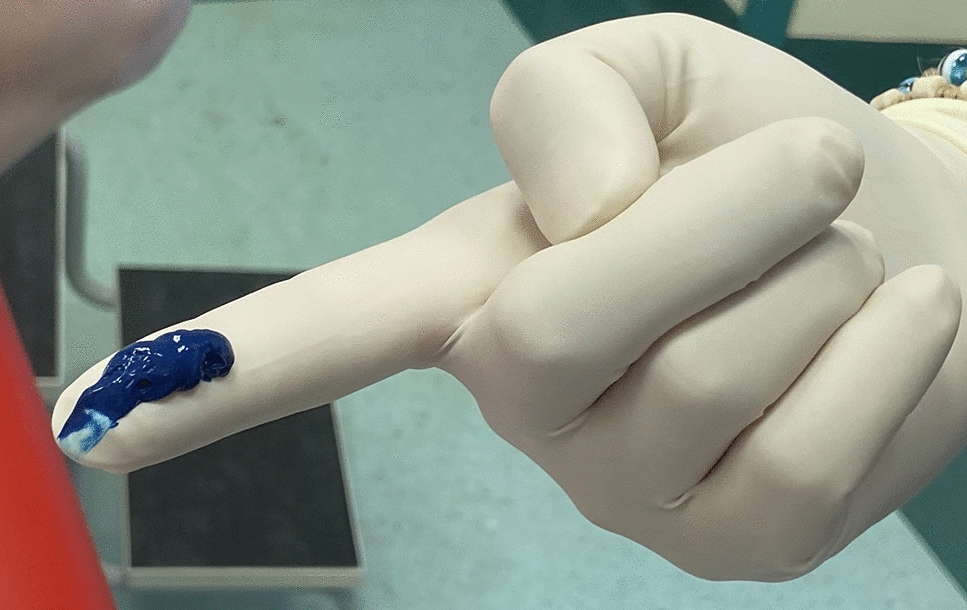
Electronic bidets or warm sitz baths were used for anal pain control and wound management after hemorrhoidectomy (Fig. 1). We developed an electronic bidet with a fountain-type water flow system that produced a lower-force water stream than commercially available electronic bidets to replace warm sitz baths (Clinic Bidet®, Coway Co., Seoul, Korea). The patients in the electronic bidet group applied the water flow of the electronic bidet around the anal wound, and the patients in the sitz bath group applied warm water around their buttocks by sitting in a small tub. The water used in the electronic bidet and sitz bath was warm tap water at approximately 38 °C. The patients were directed to use the electronic bidet or sitz bath for 3–5 min every morning for 7 days after hemorrhoidectomy. The patients could also use their allocated device several times in the daytime when they wanted to alleviate anal pain or clean the perianal wound area for 4 weeks after the operation.
Fig. 1
Electronic bidets (a) or warm sitz baths (b) were used for anal pain control and wound management after hemorrhoidectomy
Efficacy and safety assessmentThe severity of anal pain after hemorrhoidectomy was assessed by using the visual analog scale (VAS) (Figure A1). It has been used as a common measurement tool to evaluate subjective characteristics or to quantify pain. The patients recorded their VAS score before and after the electronic bidet or sitz bath every morning for 7 days after hemorrhoidectomy. The primary endpoint was the difference in the VAS score for anal pain after the use of an electronic bidet or sitz bath at 7 days after the operation to assess the efficacy of the electronic bidet for anal pain control after hemorrhoidectomy. Adherence to the procedure was assessed by checking the complete recordings of the VAS score for 7 days. The secondary endpoint was the difference in the wound healing rate at 4 weeks after the operation and the results of a comprehensive patient-reported assessment of the convenience of postoperative care, which was scored as follows: 1: completely inconvenient, 2: considerably inconvenient, 3: neutral, 4: considerably convenient, and 5: completely convenient.
Safety was assessed by the independent data monitoring committee, who monitored adverse events during the study periods. Safety evaluations included a comprehensive analysis of reported adverse events and serious adverse events. Adverse events were classified as definitely, probably, possibly, or remotely related to the interventional procedures.
Study designWe hypothesized that for the alleviation of anal pain, the electronic bidet would not be inferior to the sitz bath at 7 days after hemorrhoidectomy. Therefore, we planned a noninferiority test with a 10% difference margin, 80% power and 2.5% type I error. The effect of the sitz bath was based on the study of Gupta [21], in which the authors reported an average VAS score of 22.0 (SD: 3.2) for the sitz bath group. The test statistic used was two-sided Fisher’s exact test. The required number calculated for each group was 34.
Statistical analysisBaseline characteristics are presented as the means ± standard deviations (SD) for continuous variables and as numbers and percentages for categorical variables. A two-sided 95% confidence interval for the VAS score difference between the treatment groups was evaluated; whether the upper limit of the 95% confidence interval fell within the predetermined margin of noninferiority was checked to provide evidence of the noninferiority of electronic bidets to sitz baths. The conclusion regarding the primary outcome was based on the result from the full analysis set (FAS) population; the per-protocol (PP) analysis result was also provided. The FAS population consisted of patients who used the intervention at least once, while the PP population consisted of patients with more than 80% complete use of the electronic bidet or sitz bath according to the protocol for 7 days. Student’s t test was used to analyze the main outcome: the difference in VAS scores for anal pain. The difference in the wound healing rate at 4 weeks after the operation between the two groups was compared using the chi-square test or Fisher’s exact test, as appropriate. Statistical analysis was performed using SPSS for Windows, version 22.0 (SPSS, Chicago, IL, USA), and statistical significance was assumed for p values < 0.05.
留言 (0)