
記住我



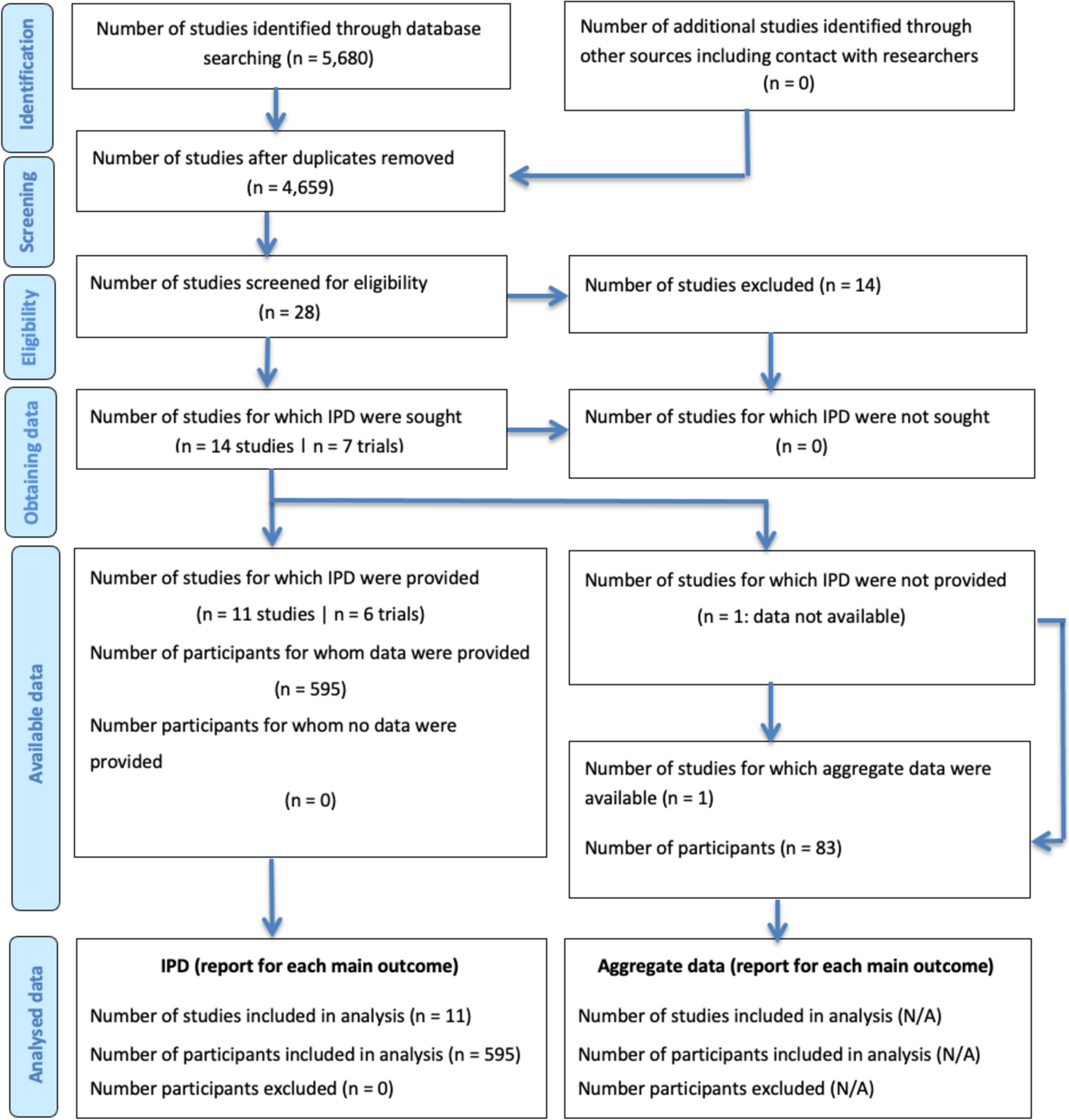
A total of 787 patients were included in the study; 534 (67.9%) men and 253 (32.1%) women were included in the analyses (see Supplementary material). Table 1 reports the characteristics of these patients. Median patient age was 67 years (IQR 59–75), body mass index (BMI) was 26.5 (IQR 23.5–29.1), and 413 (52.5%) were classified as American Society of Anesthesiologists (ASA) III or IV. Rectal cancer was classified as stage T3 in 456 patients (57.9%) and as stage N1 or N2 in 467 patients (59.3%). Tumour height from the anal verge was 10–15 cm in 257 patients (32.7%), 5–10 cm in 334 (42.4%), and less than 5 cm in 176 (22.4%); 76 (9.7%) had synchronic metastases. Neoadjuvant therapy was administered in 471 patients (59.8%).
Table 1 Patients demographic, clinical, and surgical characteristicsSurgical variables and postoperative outcomesRectal anterior resection was performed in 653 patients (82.9%), whereas abdominoperineal amputation was performed in 126 patients (16.0%). The remaining eight surgeries were six exenterations and two proctocolectomies. Anastomoses were handsewn in 67 patients (10.9%) and stapled in 548 cases (89.3%). Laparoscopy was the main surgical approach (63.7%), followed by robotic, TaTME, and laparotomy. Conversion rate was 10.6%.
Protective ileostomy was performed in 357 patients (45.4%), protective colostomy in 1 patient (0.1%), end colostomy in 169 patients (21.5%), and 260 patients were stoma-free (33%).
As shown in Table 2, 311 patients (39.5%) had early postoperative complications. Minor complications (< IIIa) were identified in 207 patients (26.3%), whereas 104 additional patients (13.2%) had major complications (≥ IIIa). Anastomotic leak was detected in 54 patients (8.8%). Eighty-five patients underwent a re-intervention (10.8%) and 81 patients were readmitted (10.3%). The median of postoperative stay was 7 (IQR 5–12) days.
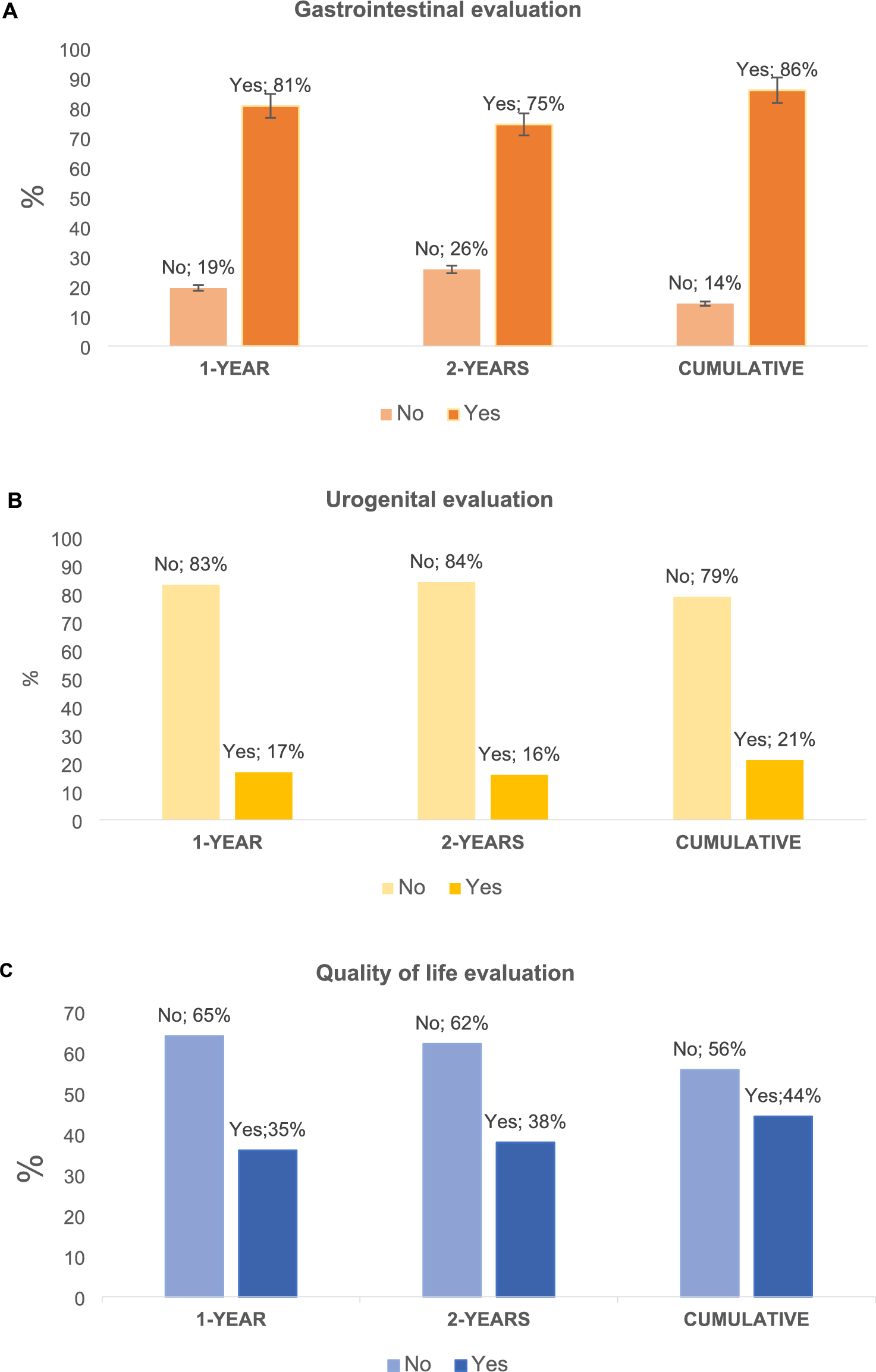
Table 2 Patients’ postoperative and tumour characteristicsClinical care assessment 1 and 2 years post surgeryTable 3 reports the clinical assessment performed by surgeons during the first and second years after surgery, and Fig. 1 shows rates according to gastrointestinal, urogenital, and quality of life evaluations. Follow-up was performed in 772 patients during the first year (15 patients were lost during follow-up) and in 729 patients during the second year (32 patients were lost during follow-up and 26 died after the first year surgery).
Table 3 Gastrointestinal and urogenital function evaluation at 1 and 2 years post rectal cancer surgeryFig. 1
Clinical care assessment at first and second year of follow-up and cumulative rates 2 years post surgery
One year after rectal cancer surgery, bowel movements per day were recorded in the medical notes of 37% of patients, fecal incontinence in 90 patients (20.1%), and LARS in 79 patients (17.6%). However, only 15.8% of patients had their LARS score measured.
Sexual and urinary function were missing in the medical notes for more than 90% and 83% of surgical patients, respectively. The use of questionnaires to assess urogenital function after surgery was 0.3% for sexual function and 0.6% for urinary function.
The impact of surgery on patients’ quality of life was recorded in only 273 patients (35.4%) and quantified through the questionnaire in just 0.8% of patients.
Prescribed treatments in patients who have experienced digestive and/or genitourinary sequelae 1 year post surgery were as follows: sacral neuromodulation, n = 9 (1.2%); rehabilitation, n = 40 (5.2%); medication, n = 144 (18.7%); and/or referral to other specialists, n = 98 (12.7%) and other treatments, n = 10 (1.3%) which include end colostomy formation, transanal irrigations, and hyperbaric chamber.
In the second year of follow-up, 172 patients (33.3%) had their bowel movements recorded in the medical notes. LARS and fecal incontinence after 2 years were recorded in 17.8% and 20.5% of patients, respectively. The LARS score was measured in 71 patients (13.7%).
Sexual function was recorded in 10.3% of patients and urinary function in 15.4%. Questionnaires to quantify urinary and sexual function after 2 years were administered to 0.4% (3 patients) and 0.1% (1 patient), respectively. There was no use of questionnaires to assess emotional and physical well-being at 2 years after surgery.
Patients who developed genitourinary and/or digestive sequelae 2 years following surgery were prescribed the following treatments: sacral neuromodulation (n = 21, 2.9%), rehabilitation (n = 47, 6.4%), medication (n = 132, 18.1%), referral to other specialists (n = 52, 7.1%), and other treatments (n = 20, 2.7%), including those mentioned previously.
At the 2-year follow-up, the number of bowel movements per day was recorded in 242 patients (46.4%). Fecal incontinence was experienced by 146 patients (28.2%), and LARS by 124 patients (23.8%). The LARS questionnaire was completed by 106 patients (20.3%) at 2 years after surgery.
Urinary dysfunction was recorded in 5.1% of surgical patients, and sexual dysfunction in 5.5%. However, sexual and urogenital function were not recorded in the medical notes for over 80% and 70% of patients, respectively.
Only 320 patients (43.9%) had their quality of life after surgery evaluated, and just 0.8% of patients completed a Quality of Life questionnaire.
Sacral neuromodulation (n = 25; 3.4%), rehabilitation (n = 68; 9.3%), medication (n = 196; 26.9%), and/or referral to other specialists (n = 110; 15.1%) and other treatments (n = 25; 3.4%), including end colostomy formation, transanal irrigations, and hyperbaric chamber, were prescribed for patients who experienced digestive and/or genitourinary sequelae 2 years post surgery.
留言 (0)