
記住我



Twenty-five videos of robotic anterior resection performed with Da Vinci™ Xi system at Champalimaud Foundation were examined. All patients signed an informed consent to imaging, video recording, and data publication. Ethical approval was obtained. Each video was assessed by a minimum of two surgeons. The intervention was segmented into modules, then further subdivided into steps. Modules represent major phases of the procedure. Steps are key moments of exposure, marked by changes in traction for dissection. Tractions are pivotal for exposure; they are classified as macro- or microtractions. A macrotraction is the grasping of structures (organ or mesentery) to adequately expose dissection areas. A microtraction is the dynamic grip or exposure of tissue to optimize macrotractions and guide dissection paths.
In multimedia content, robotic first arm instrument tractions are depicted in green, those by the fourth arm in blue, and laparoscopic assistant ones in yellow. Table 1 summarizes the modules.
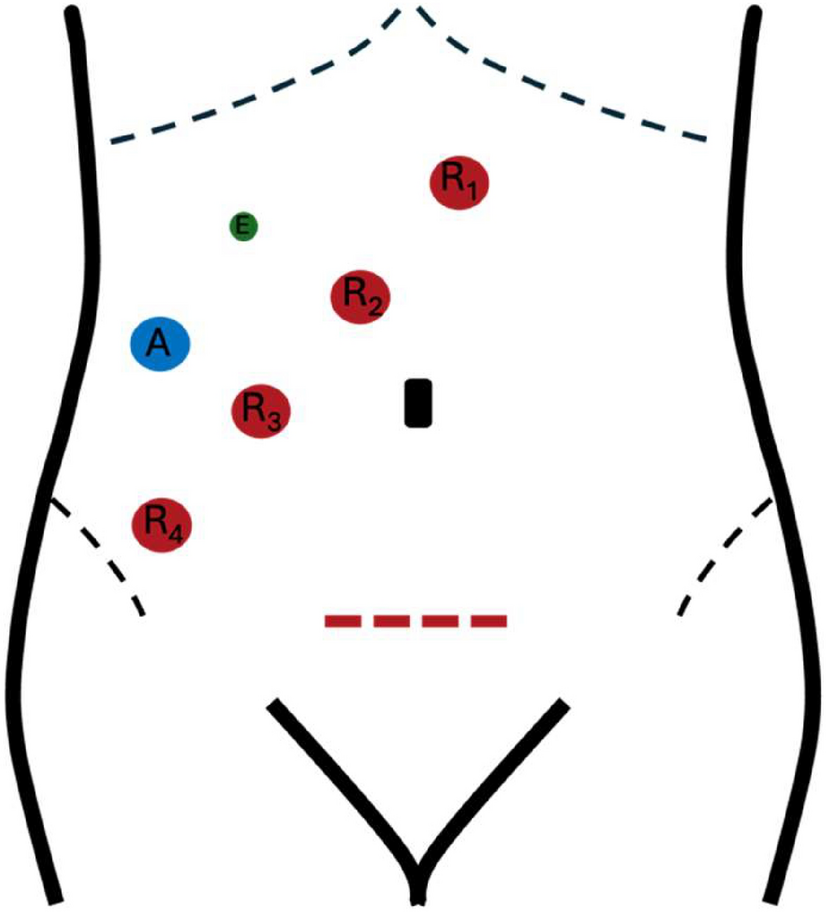
Table 1 Modular division of robotic low anterior resection with TMEPatient setup and positioningThe patient is in Lloyd-Davis position, with a Trendelenburg tilt of approximately 20–22° and rotated about 8–10° to the right. A Pfannenstiel incision is made for specimen extraction; four robotic trocars are placed 6–8 cm apart on a diagonal line from the right lower quadrant to the epigastrium on the right of the umbilicus (Fig. 1). An assistant trocar aligns with the third robotic trocar in the right lower quadrant, where AirSeal® is utilized. An additional 5-mm assistant port may be needed for lower tumors and complex cases.
Fig. 1
Robotic setup. The Pfannenstiel incision is depicted by a dotted red line, the robotic trocars are drawn as red dots along a diagonal line from the right lower quadrant to the epigastrium with a 6–8 cm distance between one another, the assistant trocar is represented with a blue dot, and an eventual additional trocar is represented in green
Module 1—surgical field exposureTo start the procedure, exploratory laparoscopy to exclude metastatic spread of the disease is necessary. Exposure of the surgical field (video 1):
1.Adhesiolysis may be necessary, according to patient conditions and previous surgical history.
2.Greater omentum is gently positioned, without traction, in the left hypochondrium.
3.Small bowel loops are swept, without grasping, to the right abdominal quadrants, firstly near the Treitz, exposing the origin of the inferior mesenteric vessels, secondly to the right lower quadrant.
4.A gauze is placed to maintain the position of the bowel loops at the ligament of Treitz (Fig. 2a).
5.An additional gauze can displace the bowel loops in the lower right abdomen to expose the pelvis (Fig. 2b).
Fig. 2
Surgical field exposure. A gauge is used to maintain small bowel loops on the right abdomen, the assistant forceps applies a pressure upward at the level of the ligament of Treitz to expose the mesentery of the left colon (a); an additional gauge can be used and placed in the lower right abdomen to keep bowel loops away from the operating area (b); docking is performed (c)
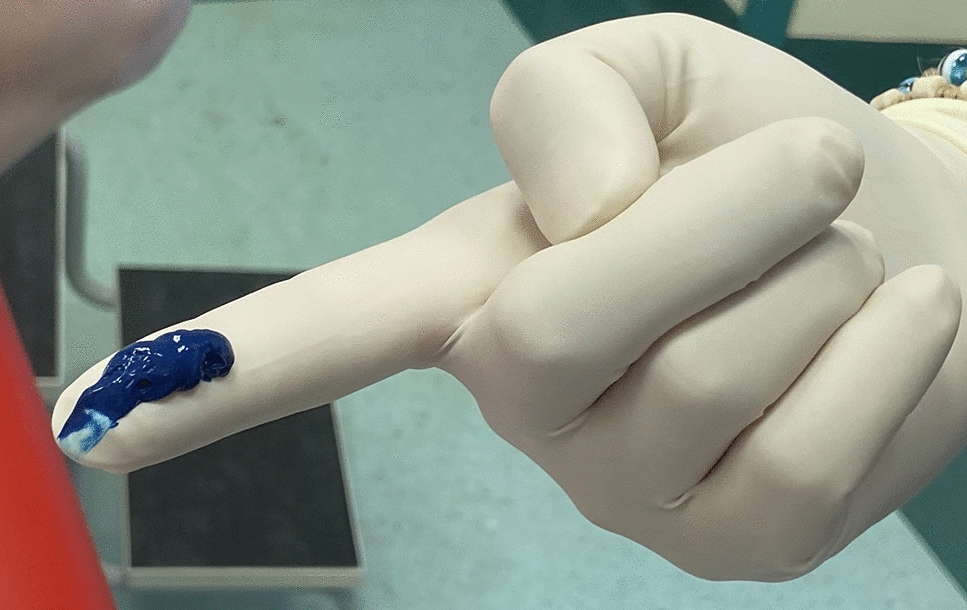
At the end of this module, docking (Fig. 2c) of the robot is performed. The suggested setting for the instruments is the bipolar fenestrated forceps in arm 1, the robotic camera in arm 2, the monopolar curved scissors on arm 3, and the Cadière forceps in arm 4.
Module 2—approach to the inferior mesenteric vessels and lymphadenectomyModule 2.1—inferior mesenteric artery (IMA) ligationStarting the procedure with proper exposure is key to initiate dissection in the correct plane. This module is represented in video 1.
1.Exposure of the mesocolic root is obtained with a macrotraction by arm 4 on the sigmoid colon upward to extend the peritoneum and distance it from retroperitoneal structures (Fig. 3a). An up-and-down movement may highlights the dissection plane with sliding of the retroperitoneal fascia covering the structures.
2.The first arm applies microtraction (Fig. 3b) on the mesentery cranially and medially for exposure of the IMA.
3.The macrotraction and the optimizing microtraction expose the IMA archiform projection on the mesenteric surface (Fig. 3c). Dissection separates the mesocolon from the retroperitoneum.
4.The macrotraction of arm 4 moves proximally on the arch of the IMA to increase tension on the vessel. This allows skeletonization and high ligation of the IMA. A first-arm microtraction makes IMA isolation easier (Fig. 3d).
5.The first arm slides below the artery to facilitate dissection at the origin of the vessel (Fig. 3e). The correct plane of dissection below the artery is identified for retroperitoneal dissection.
6.To obtain complete IMA skeletonization, the window below the inferior mesenteric vein (IMV) can be opened (Fig. 3f). The first arm grasps the peritoneum at the projection of the IMV. The planes of dissection below IMV and IMA are connected around the IMA.
7.The first-arm applies finest microtraction upward and laterally counteracts the force of the scissors to open the space behind the artery at its origin (Fig. 3g). As evident in Fig. 3h, this step can be performed by inverting the forces from the two arms.
8.Once skeletonization is completed, IMA is ready for ligation. The scissors apply a microtraction directly on the artery upward and laterally, parallel to the macrotraction, allowing arterial clipping by the assistant operator (Fig. 3i). A gauze can be positioned posterior to the arterial origin for safe ligation.
9.This double macro- and microtraction at the level of the artery enables adequate high-level ligation, with two locking clips (Hem-o-loks) at 1 cm from aortic origin to avoid damage to sympathetic nerve trunks (Fig. 3j). High ligation guarantees accurate lymphadenectomy.
10.The microtraction of the scissors is displaced more distally to allow for distal clip closure (Fig. 3k). After the clip applier is in place, scissors are removed, and the clip is positioned distally on the vessel.
11.For vessel section, arm 1 microtraction is performed distally to the distal clip (Fig. 3l).
Fig. 3
Approach to the IMA. Step by step (a–l) exposure techniques with depiction of macro- and microtractions for isolation and ligation of IMA
Module 2.2—inferior mesenteric vein (IMV) ligationThe ligation of the IMV is crucial in left colon mobilization (video 1). In general, the site of ligation of the IMV is at the level of the ligament of Treitz, below the inferior border of the body of the pancreas.
1.The first arm grasps the peritoneal surface at the IMV (Fig. 4a). This microtraction exposes the vein (Fig. 4b) and the dissectable mesocolic plane. Arm 4 pulls the vein upwards and distally (macrotraction) to increase vein exposure, cranial to the artery.
2.The first arm slides below the vessel, supporting it, and continues to exert traction for innermost mesocolic plane dissection from medial to lateral (Fig. 4c). IMV is isolated and skeletonized.
3.As for IMA isolation, the first arm pulls upward (fine microtraction) for passage of the scissors around the IMV (Fig. 4d, e).
4.The assistant applies a pressure on the gauze for field exposure, facilitating IMV complete visualization and ensuring distance from the left colic vein. To ligate the vessel (either two or one proximal and one distal locking clips), the scissors perform a microtraction, aligned to the fourth arm, sliding below the vessel distally (Fig. 4f).
5.To optimize traction on the vein for section, arm 1 exerts a microtraction distal to the distal clip, or proximal to the clips (Fig. 4g). The vein is sectioned.
Fig. 4
Approach to IMV. Step-by-step (a–g) exposure techniques with depiction of macro- and microtractions for isolation and ligation of IMV
Module 3—medial to lateral dissection of left and sigmoid mesocolonOnce vessels are ligated, medial to lateral dissection on the innermost dissectable plane of the left colon mesentery is performed (video 2).
1.The fourth arm exerts a macrotraction at the level of the IMV, proximal to the site of IMA ligation, directed caudally and upward; the first arm guides the dissection applying a dynamic microtraction upward, above the dissection plane. The assistant grasps Gerota’s fascia, exerting a counter-microtraction (Fig. 5a, yellow). The innermost dissectable plane is revealed, outlined in white in Fig. 5b. This step is dynamic. Dissection advances while microtractions are displaced laterally. The white line of Toldt is exposed (Fig. 5c). Cranially, the inferior border of the pancreas is dissected from the left mesocolon.
2.Moving caudally, below the site of ligation of the IMA, arm 4 slides below IMA, and arm 1 moves below the mesentery, cranially to the fourth arm. These tractions allow for mesentery tenting. Retroperitoneal dissection is performed by sweeping with scissors on the fascia.
3.The plane of dissection above and below IMA origin are united, and complete mesentery tenting is obtained. Left gonadal vessels and left ureter are preserved (Fig. 5d). A gauze can be placed below the mesentery.
4.Dissection should continue to the sacral promontory, if straightforward from this position.
Fig. 5
Medial to lateral dissection. Key exposure steps (a–e) for medial to lateral dissection
Module 4—lateral colon mobilizationAt completion of medial to lateral mobilization, when the left colon is visible, lateral dissection is started (video 2). In most of the videos analyzed, lateral dissection follows medial mesentery dissection. Sometimes, lateral dissection is approached first, e.g., very fatty mesenteric planes, mesentery adherent to retroperitoneal structures, previous inflammation of left or sigmoid colon.
1.The fourth arm stretches the lateral parietal peritoneum at the passage of the descending to sigmoid colon. Meanwhile, dynamic traction is performed by the first arm on the fat of the left colon, thus the plane of dissection is displayed (Fig. 6a).
2.The dissection of the left colon mesentery from the parietal peritoneum proceeds in a caudal to cranial direction with continuous traction. A methaphorical image to represent the surgeons’ hand movements is that of “opening a book” (Fig. 6b). The two hands perform an internal to external rotation. To optimize tissue exposure, an additional traction can be applied by the assistant on the left colon (Fig. 6c). If a gauze was positioned medially, when lateral dissection reaches the medial, it is displayed (Fig. 6d).
Fig. 6
Lateral to medial dissection. Key exposure steps (a, b) for lateral to medial dissection and connection with the medially dissected plane (c)
Module 5—splenic flexure takedownBefore starting splenic flexure takedown, robotic arms are rotated, without docking, in a counterclockwise direction to the maximum range. This rotation enables splenic flexure mobilization without arm collision. Two approaches may be performed for splenic flexure takedown. One starts from lateral mobilization and follows the colon until entering the lesser sac. The second approach starts medially, in the transverse colon, and proceeds with the separation of the greater omentum from the colon from medial to lateral before entering the lesser sac. The steps for lateral approach exposure (video 2) can be described as follows:
1.The book-opening maneuver is continued to detach the splenic flexure from lateral attachments (Fig. 7a). The fourth arm is moved to the parietal peritoneum lateral to the splenic flexure. The first arm pulls downward and medially the colon. In this step, the assistant forceps performs an additional traction, equivalent to the one of arm 1 forceps, on the transverse colon.
2.Moving medially, the first arm grasps the greater omentum perpendicular to the transverse colon, the assistant pulls downward the colon; in this way the plane of dissection, close to the bowel wall, is exposed (Fig. 7b). Colo-epiploic detachment is performed. The lesser sac is opened (Fig. 7c). The dissection proceeds laterally connecting with the mesenteric planes dissected laterally and medially.
3.At the level of the attachment to the splenic hilum—or pancreatic tail—traction is performed on the flexure mesentery, gradually dissecting in a centripetal direction (Fig. 7d).
Fig. 7
Splenic flexure takedown. Key exposure steps (a, c) for splenic flexure mobilization, from lateral (a) to medial approach with colo-epiploic detachment and opening of the lesser sac (b, c) and final takedown of the splenic flexure (d)
Module 6—proctectomy with total mesorectal excision (TME)TME represents the most challenging phase of this intervention (video 3). The ergonomic advantages provided by the robotic platform facilitate it.
1.The first approach to TME is posterior. The assistant supports the colon, pulling it upward. The fourth arm grasps the sigmoid–rectal junction and extends it upwards–vertically. The first arm slides below the colon to support it. Mesorectal dissection begins posteriorly in between the hypogastric nerves (Fig. 8a). The dissection proceeds downward in the pelvis, centrally, on the innermost dissectable plane. A tunnel is created by the tension of the surrounding tissues (Fig. 8b). The plane of dissection is ventral to the presacral fascia and to Waldeyer’s fascia starting from S2–4. These anatomic landmarks grant safe dissection, avoiding bleeding from presacral veins.
2.When posterior dissection becomes tunneled, lateral dissection is started. The fourth arm releases the colon, arm 1 exerts a microtraction directed rightward on the rectal wall to expose the right border of the peritoneal reflection, which is marked (Fig. 8c). Dissection of the mesorectum continues to the right side and posteriorly, connecting the two planes. To expose the area, arm 4 is positioned on the right pelvic wall, straining the parietal peritoneum (Fig. 8d). The left hypogastric nerve is visualized and carefully preserved (Fig. 8e).
3.Dissection progresses anteriorly, the peritoneal reflection is marked, then mesorectal dissection starts. The fourth arm tractions the anterior parietal peritoneum below the pubis. The first arm pulls the rectal visceral peritoneum downward centrally (Fig. 8f).
4.Anteriorly, Denonvilliers’ fascia [9] is found, a membranous lamina that continues with the peritoneal cul de sac. For non-anterior rectal tumors, Denonvilliers’ fascia is sectioned (Fig. 8g) below the level of seminal vesicles in male; the plane of dissection is located immediately dorsal to it. The first arm microtraction is exerted on the mesorectum downward and centrally.
5.Mesorectum mobilization is obtained when anterior and posterior planes join by left lateral dissection (Fig. 8j). To achieve this, the fourth arm tractions laterally the left parietal peritoneum. First Arm 1 pulls to the right the peritoneal reflection (Fig. 8h) and secondly to the left mesorectum. The first arm dynamic traction opens the plane of dissection (Fig. 8i). With a slow and continuous increase in traction on the mesorectum, the neurovascular bundle is freed from the mesorectum.
6.When approaching the lower portion of the mesorectum posteriorly, traction on the posterior mesorectum is performed upward by the fourth arm forceps, below the rectosigmoid junction. This can be called the “hockey-stick” maneuver because of the position of the articulated forceps, as seen in Fig. 8k. This traction allows for visualization of the so-called Bill’s buttocks, after complete freeing of the mesorectum.
7.Dissection continues distally until it reaches the pelvic floor. The robotic camera is inverted to optimize vision. The first arm applies a microtraction on the posterior mesorectal fascia and exposes the anococcygeal ligament (Fig. 8l) [10]. Careful entry in the pelvis by the instruments is crucial at the pelvic inlet with the sacral promontory.
8.Rectal wall exposure is performed circumferentially at the level defined for section. The first arm retracts the rectal wall for isolation (Fig. 8m).
Fig. 8
Total mesorectal excision. Key exposure steps (a–m) for proctectomy with TME
Module 7—rectal transection 1.In a female patient, the fourth arm supports the uterus upward; the first arm tractions posteriorly the rectal wall (Fig. 9a) so the robotic stapler is positioned at the level of transection.
2.In a male patient, the Cadière forceps exposes anteriorly the pelvis (Fig. 9b). The instrument may be replaced by a Tip-Up grasper when extra exposure in a deep pelvis is needed.
3.Rectal transection is completed by stapler firing. The fourth arm widens the pelvis by tractioning the peritoneal fold anteriorly; arm 1 calibrates the direction of the rectum for stapling. Firing is performed in an anterior to posterior direction (Fig. 9c). More than two firings should be avoided.
Fig. 9
Rectal transection. Exposure of the female pelvis (a) and of the male pelvis (b). Linear stapling of the distal rectum (c)
This module is displayed in video 3.
Module 8—anastomosisAfter stapling, the mesentery is sectioned and bowel perfusion can be checked by real-time angiography; these steps can be performed extracorporeally. Proximal section of the colon is performed extracorporeally. The anvil is secured, and the colon is repositioned intracorporeally. Anastomosis is performed (video 3).
1.The colon is brought to the pelvis.
2.For the anastomosis, the fourth arm grasps the stapler anvil (Fig. 10a). The assistant, or arm 4, exposes the pelvis by applying a macrotraction anteriorly on the parietal peritoneum.
3.Checking for proper mesentery orientation is fundamental before anastomosis sealing (Fig. 10b, c).
4.Circular end-to-end stapled tension-free anastomosis is performed (Fig. 9d).
Fig. 10
Anastomosis. Colon positioning in the pelvis (a), correct mesentery orientation checking (b, c), and anastomosis construction (e)
留言 (0)