This is a comprehensive study to describe the incidence and rates of change of T2DM among adolescents and young adults aged 10–24 years across 200 countries and territories from 1990 to 2021, analyzed at the global, regional, and national levels. A slowing trend in the increase of T2DM incidence among this demographic has been observed since 2009, which may be associated with global efforts in T2DM management. While the overall global incidence of T2DM among adolescents and young adults increased between 1990 and 2021, significant stabilization in the growth rate was observed between 2009 and 2017 (APC 1.25). This rate was about one-third of the increase rate observed from 2002 to 2009 (APC 3.54) and from 2017 to 2021 (APC 3.57). In 2021, male adolescents and young adults accounted for more than half of the incident T2DM cases. The AAPC in mortality from 1990 to 2021 was nearly four times higher in females compared to males. Adolescents aged 15–19 years had an AAPC for T2DM mortality more than 2.4 times that of the 20–24 age group during the same period. However, from 2010 to 2021, young adults aged 20–24 years exhibited a significantly higher AAPC for T2DM mortality. Between 1990 and 2021, the highest increase in T2DM incidence among adolescents and young adults was observed in North Africa and the Middle East. High SDI countries also demonstrated the largest increase in T2DM incidence within this age group.
T2DM is a significant global public health concern, leading countries to implement various strategies and policy guidelines to manage and control the disease. Efforts to combat T2DM include public health campaigns, healthcare infrastructure improvements, and patient education programs. To provide a clearer roadmap for policymakers and public health practitioners, we propose several targeted intervention strategies: (1) implementing school-based and community-wide programs to promote healthy eating and physical activity among children and adolescents; (2) strengthening primary healthcare systems to ensure early diagnosis and continuous management of T2DM, especially in high-risk groups; (3) developing culturally tailored education and awareness campaigns that address specific local risk factors, including dietary habits and sedentary lifestyles; and (4) integrating digital health solutions, such as mobile apps and telemedicine, to improve patient engagement and adherence to treatment plans. These strategies can help guide effective policy implementation and reduce the global burden of T2DM. Based on the GBD data from 2021, the positive percentage contribution of risk factors to DALYs for T2DM among adolescents and young adults aged 10–24 worldwide is ranked as follows: high fasting plasma glucose, metabolic risks, high body-mass index, environmental/occupational risks, suboptimal temperature, high temperature, and low temperature. Among these, high fasting plasma glucose and metabolic risks emerge as the most significant contributors to the burden of T2DM, substantially surpassing other factors. These findings suggest that comprehensive interventions targeting these primary and secondary risk factors are crucial for reducing the burden of T2DM among adolescents and young adults.
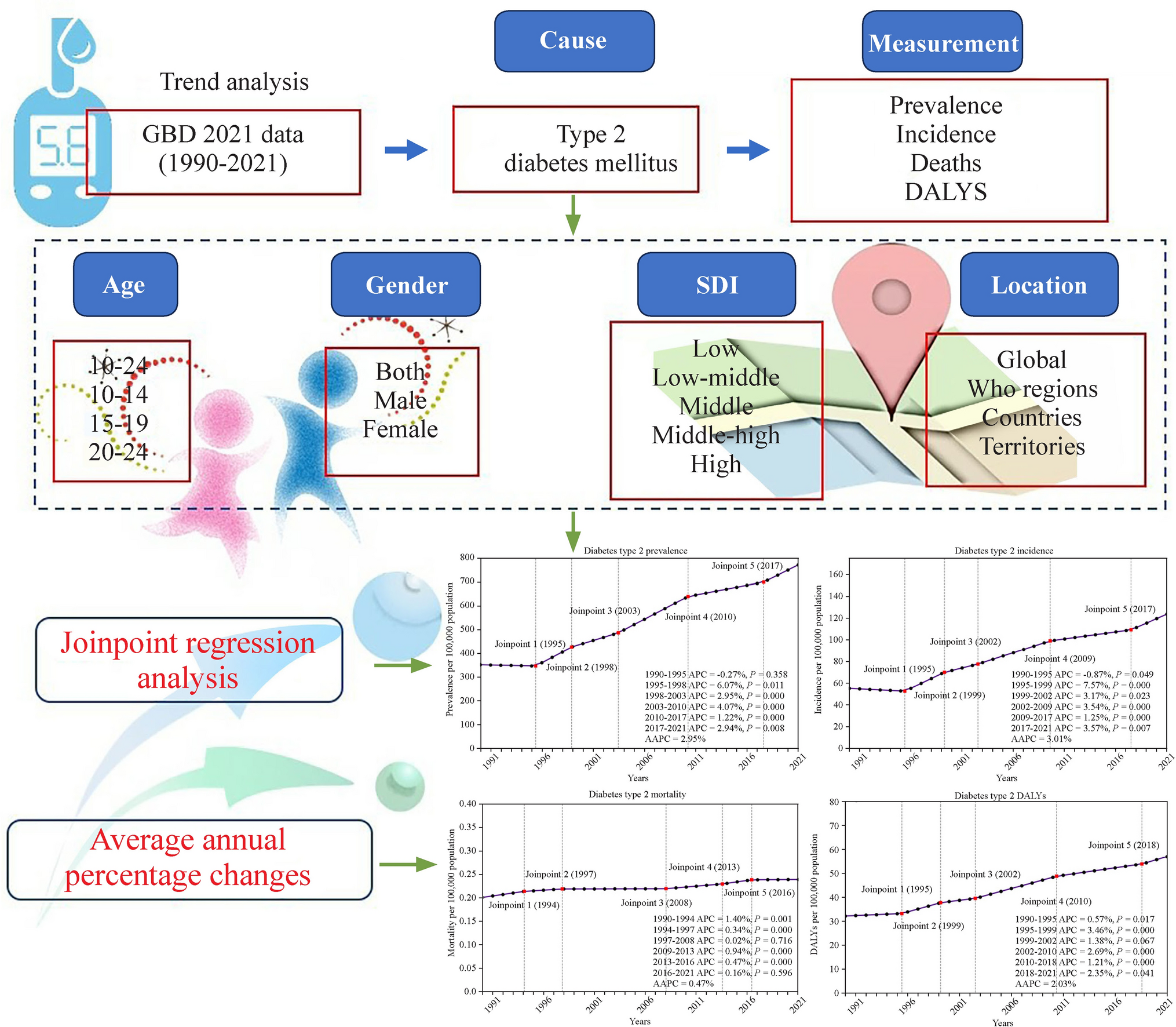
Significant stabilization in growth rates was observed at key joinpoints: prevalence in 2010, incidence in 2009, and DALYs in 2010, coinciding with the introduction of global T2DM management strategies. In the USA, the American Diabetes Association (ADA) releases annual guidelines to help healthcare providers in managing diabetes. The 2009 Standards of Medical Care in Diabetes emphasized personalized patient care, the integration of technology, and lifestyle management to improve blood sugar control and reduce complications [22]. In the UK, the National Health Service (NHS) launched the NHS Diabetes Prevention Programme in 2010, aiming to prevent T2DM through lifestyle interventions and support for high-risk individuals. The success of this program has led to its expansion and integration into routine healthcare services [23]. Australia has also made significant strides with the National Diabetes Strategy 2010–2020, focusing on early detection, effective management, and support for research into diabetes prevention and treatment. This strategy underscores the importance of community-based programs and the role of primary healthcare providers [24]. In China, the Ministry of Health released guidelines in 2010 to standardize diabetes prevention and control, including early diagnosis, patient education, and integration of diabetes care into the broader public health system [25]. From 2017 to 2021, there was a renewed moderate increase in T2DM incidence among adolescents, which may be partly attributed to the ongoing obesity epidemic and potential impacts of COVID-19. Rising obesity rates among children and adolescents have significantly influenced T2DM incidence [26]. This partly explains why the AAPC of T2DM mortality in the 15–19 age group was more than 2.4 times that of the 20–24 age group between 1990 and 2021. However, from 2010 to 2021, the AAPC of mortality in the 20–24 age group was significantly higher than that in the 15–19 age group, suggesting a need for targeted T2DM screening among young adults and adolescents. The COVID-19 pandemic appears to be associated with an increase in new-onset T2DM cases in children and higher hospitalization rates in 2020 compared to 2019; however, further studies are needed to differentiate the direct effects of the pandemic from other contributing factors, such as reduced physical activity and changes in diet [27,28,29]. The pandemic also caused economic and social disruptions, affecting access to healthcare and worsening existing health disparities [30, 31].
From 1990 to 2021, the most significant increase in T2DM incidence among adolescents and young adults occurred in the 15–19 age group. This increase is primarily attributed to hormonal changes during puberty, lifestyle factors such as increased consumption of high-calorie foods, and reduced physical activity. Additionally, socioeconomic disparities affect access to healthcare and healthy food options [32, 33]. The 20–24 age group also experienced a notable rise in T2DM prevalence and DALYs, which may be influenced by factors such as the transition to independent living, educational and occupational stress, and delayed healthcare access. Although the 15–19 age group experienced a higher overall increase in mortality, the 20–24 age group experienced a significant rise in mortality rates between 2010 and 2021. This reflects challenges in managing the transition from pediatric to adult healthcare systems and the chronic nature of diabetes complications [34].
We identified a sex disparity in T2DM among adolescents and young adults. Studies indicate that T2DM incidence and prevalence are higher in adolescent males compared to females [35]. Despite this, females with T2DM exhibit higher DALYs and mortality rates [36]. Notably, our study found female mortality rates to be four times higher than those of males. The increased T2DM incidence in males is attributed to biological and behavioral factors. Hormonal differences, such as the influence of androgens, affect insulin sensitivity and fat distribution, thereby increasing diabetes risk in males [37]. Additionally, adolescent males are more likely to consume sugary drinks and engage in less physical activity than females [38]. Conversely, the higher DALYs and mortality rates in females result from delayed diagnosis, less aggressive treatment, higher susceptibility to complications, and psychosocial factors like depression, which adversely affect diabetes management [36]. Addressing these disparities requires targeted interventions, including early screening and diagnosis, gender-sensitive health education, and comprehensive mental health support for females with T2DM. The gender differences in T2DM underscore the need for gender-specific public health interventions. Understanding these disparities is crucial for developing effective strategies to reduce the T2DM burden.
Regionally, North Africa, the Middle East, East Asia, and North America experienced the most notable rises in T2DM incidence among adolescents between 1990 and 2021. These trends are primarily driven by rapid urbanization, dietary shifts towards high-calorie, processed foods, and reduced physical activity. To address these regional disparities, it is crucial to develop targeted interventions such as improving urban planning to increase access to recreational spaces, providing subsidies for healthier food options in areas with limited access, and launching region-specific campaigns that promote traditional diets and active lifestyles. These strategies should be adapted to the unique socioeconomic and cultural contexts of each region to maximize their effectiveness. Economic development and lifestyle changes, such as increased consumption of western diets and sedentary behavior, further contribute to the increasing incidence. In North America, the obesity epidemic, characterized by high fast-food consumption and low physical activity, plays a crucial role in the rise of T2DM incidence [34]. Socioeconomic disparities also impact access to healthcare and preventive services, exacerbating T2DM management challenges. Southern Sub-Saharan Africa had the highest T2DM incidence rate in 2021, along with a significant increase in mortality. Factors such as limited healthcare access, poor nutrition, and high rates of infectious diseases complicate diabetes management in this region [39]. High-income regions, particularly Southern Latin America, showed the largest increase in T2DM prevalence. North America experienced the largest increase in DALYs due to T2DM, reflecting the chronic nature of diabetes and the burden of related complications. The rapid spread of T2DM among adolescents and young adults in high-SDI quintile countries requires urgent attention. Addressing these regional disparities necessitates targeted interventions, including improved healthcare access, promotion of healthy lifestyles, and effective public health policies tailored to specific regional needs. Nationally, efforts should focus not only on countries with the highest current T2DM burdens, but also on those experiencing rapidly increasing burdens, as unprepared countries are particularly vulnerable to epidemics. Although the widespread T2DM epidemic among adolescents and young adults in lower SDI countries has prompted global and local efforts, the rapid spread in high and middle-high SDI countries also requires urgent action.
The strength of the current study lies in its provision of an up-to-date epidemiological analysis of the global trend of T2DM based on the GBD 2021 findings. This report not only includes the four classic measures—prevalence, incidence, mortality, and DALYs—but also their changing trends at global, regional, and national levels. Additionally, it employs AAPC modeling to estimate the independent effects of age, gender, and region, thereby presenting a clear and multidimensional picture of the T2DM burden over the past three decades.
Our study has several limitations. Firstly, the results are influenced by the methods used in the GBD 2021. In cases of missing data, results relied on predictions from the model, and when data were available, preferred definitions or methods might not have been consistently used, leading to variability, such as in the definition of T2DM across different data sources. This variability may introduce bias in estimating T2DM incidence and mortality rates, potentially leading to either overestimation or underestimation depending on the data source. While techniques were implemented to minimize bias in the GBD 2021, complete elimination of bias is not feasible, meaning the direction of this potential bias could vary, and the magnitude of its impact remains uncertain. Moreover, we used confidence intervals instead of uncertainty intervals after age standardization, which may not fully capture the range of variability in our estimates. This choice could result in a narrower representation of potential outcomes; hence, our findings should be interpreted cautiously, given the possibility of underestimating the true uncertainty. Further real-world studies are needed for validation to better understand the range and impact of these estimates. Secondly, our analysis excluded children and adolescents under 15 years, as the GBD 2021 set 15 years as the age threshold for T2DM. Since T2DM is uncommon in those under 15, we believe that including this age group would not have significantly changed our main findings. Thirdly, the burden of early-onset T2DM depends on detection methods, screening quality, and data registries, all of which vary by socioeconomic level. These variations may lead to systematic biases; for example, countries with more robust healthcare systems may report higher incidence rates due to better detection, while countries with less developed healthcare services might underreport cases, leading to an underestimation of early-onset T2DM in countries with low socio-demographic indices. The direction of this bias is likely toward underestimation in low-resource settings, and the magnitude could be substantial, depending on disparities in healthcare access and data reporting. Fourthly, GBD data may have constraints in economically disadvantaged countries, which often suffer from data scarcity, incompleteness, and potential inaccuracies due to variations in data availability and quality. Despite potentially high T2DM incidence rates in these areas, the sparse data can lead to underestimation or overestimation of the true burden. Consequently, findings based on this data should be interpreted with caution. Fifthly, while our manuscript addresses variations by gender and age, it lacks a more nuanced analysis of specific populations, such as different ethnicities and socioeconomic backgrounds. T2DM incidence and mortality rates in these populations may be influenced by a range of factors, including socioeconomic status, cultural practices, and access to healthcare. We acknowledge that a deeper analysis of these specific subgroups could provide more granular epidemiological insights into the global burden of T2DM. Therefore, future research should aim to perform more detailed analyses of these populations to address this limitation.
In conclusion, the study reveals a marked increase in global incidence and burden of T2DM among adolescents and young adults from 1990 to 2021, with significant regional and demographic disparities. These trends highlight the need for targeted, region-specific interventions, especially in areas with rapid increases. The findings call for urgent policy modifications and early screening programs to address the rising T2DM burden in this vulnerable population.

留言 (0)