
記住我
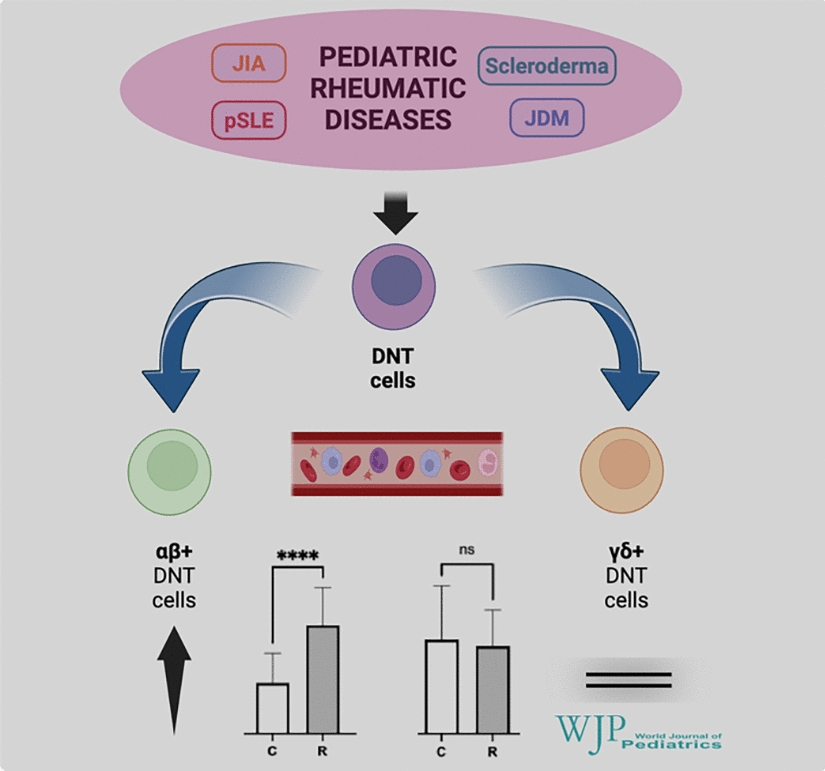


A total of 110 children with rheumatic diseases were prospectively enrolled in this preliminary study. Most patients were diagnosed with juvenile idiopathic arthritis (JIA; n = 86; 78.2%), whereas a minor part is represented by pediatric SLE (pSLE) (n = 12; 10.9%) or other rheumatic disorders (n = 12; 10.9%). A detailed diagnostic classification of rheumatic children is described in Table 1. In addition, 40 control patients were recruited as a comparison group for the specific FACS analysis, particularly for DNT cells. The gender distribution (male/female ratio) was comparable between rheumatic and control groups (45/65 vs. 18/22; P > 0.05). However, the age [Me (IQR)] of controls was significantly lower than that of the rheumatic children [7.65 (3.350, 11.65) vs. 12.4 (7.25, 15.53) years; P < 0.001].
Table 1 Disease classification of rheumatic patientsRheumatic patients were subjected to variable therapeutic regimens, including non-steroidal anti-inflammatory drugs (NSAIDs), steroid drugs (SD), conventional disease-modifying anti-rheumatic drugs (cDMARDs), and biological disease-modifying anti-rheumatic drugs (bDMARDs) (Table 2).
Table 2 Ongoing therapies at the time point of the blood analysisMain hematological laboratory parametersThe complete cell blood count of children with rheumatic diseases is reported in Supplementary Table 1, where these hematological parameters are compared with those shown by controls. Notably, there is no difference in the absolute lymphocyte count between rheumatic and control patients [2.955 (2.510, 4.070) × 109/L vs. 3.025 (2.293, 3.435) × 109/L, respectively; P = 0.4515], which is important for the accurate interpretation of differences in absolute counts of specific lymphocyte subsets, including DNT cells. Among the inflammatory parameters, erythrocyte sedimentation rate (ESR) was available for the study participants. As expected, rheumatic patients showed a mild increase in ESR compared to controls [15.0 (6.5, 24.5) mm/h vs. 7.0 (4.2, 11.5) mm/h, respectively; P < 0.001].
With regard to the general lymphocyte subpopulations (Supplementary Table 2), rheumatic children showed an increased number of T cells with a greater expansion of CD8+ T cells, as also evidenced by the CD4/CD8 lymphocyte ratio [R: 1.420 (1.010, 1.780), C: 1.783 (1.410, 2.209); P < 0.001]. Conversely, a significant reduction of NK cells was observed in rheumatic children compared to controls. B cells were also slightly reduced in rheumatic children, which was mildly significant only when expressed as a relative (percentage) count.
Double-negative T cells in rheumatic children and controlsOverall, the circulating DNT cell pool (defined as any T cell lacking both CD4 and CD8 markers) was not different in rheumatic children compared to the controls, as shown in Fig. 2a. However, when analyzed according to TCR type, it was evident that children with rheumatic disorders exhibited a significant increase in the number of αβ+DNT cells compared to controls (Fig. 2b), whereas this difference is not present in the γδ+DNT cell population (Fig. 2c).
Fig. 2
Comparison of DNT cells (a) and their two main subsets, αβ+DNT cells (b) and γδ + DNT cells (c) between rheumatic children and controls, along with ROC analysis related to the count of αβ.+DNT cells (d). DNT double-negative T, TCR T cell receptor, ROC receiver operating characteristic curve, NS not significant, * P < 0.001
In detail, regarding the αβ+DNT cell subset, this difference is observed regardless of the method used to count this population, whether as a percentage of total lymphocytes [R: 0.950 (0.730, 1.283)%; C: 0.445 (0.312, 0.707)%; P < 0.001], as a percentage of CD3+(T) lymphocytes [R: 1.440 (1.080, 1.935)%; C: 0.730 (0.5025, 1.195)%; P < 0.001], or as an absolute cell count [R: 28.92 (18.60, 42.14) × 106/L; C: 13.70 (9.54, 19.20) × 106/L; P < 0.001].
To further validate this significant difference in αβ+DNT cell numbers between rheumatic children and controls, corresponding ROC curves were generated for all three modes of cell counting: percentage of total lymphocytes [AUC = 0.8527, 95% confidence interval (CI) = 0.7851–0.9203; P < 0.001], percentage of CD3+(T) lymphocytes (AUC = 0.8314, 95% CI = 0.7574–0.9054; P < 0.0001), and absolute cell count (AUC = 0.8163, 95% CI = 0.7418–0.8907; P < 0.0001, Fig. 2d).
Sub-analysis of αβ+ double-negative T cells in pediatric rheumatic diseasesJIA patients represent the majority of our study population in this preliminary research. Figure 3 shows that all JIA subtypes are characterized by a statistically significant increase in αβ+DNT cells compared to the controls, but no difference is present among the subtypes themselves. Moreover, no significant difference in circulating αβ+DNT cells was observed between JIA patients, pSLE patients, and children affected with other rheumatic diseases. However, αβ+DNT cells were increased in all these groups of rheumatic children compared to controls (Fig. 3b).
Fig. 3
Comparison of αβ+DNT cells among different JIA subtypes (a) and rheumatic diseases (b), and covariation analysis of αβ.+DNT cells according to inflammatory markers and disease activity/stage parameters (c). DNT double-negative T, JIA juvenile idiopathic arthritis, oJIA oligoarticular JIA, pJIA polyarticular JIA, PsA psoriatic JIA, ERA enthesitis-related arthritis, sJIA systemic JIA, uJIA undifferentiated JIA, pSLE pediatric systemic lupus erythematosus, ESR JADAS-10 juvenile arthritis disease activity index, SLEDAI SLE disease activity index, NS not significant, *P < 0.05, † P < 0.01, ‡ P < 0.001
As mentioned, rheumatic children could be recruited at different stages of their disease course and were also subjected to variable therapeutic regimens. We analyzed the impact of these ongoing therapeutic regimens on the main lymphocyte subsets and, in detail, on the αβ+DNT cells (Table 3). We did not observe any significant differences based on the administration of steroids, cDMARDs, bDMARDs, or their combinations.
Table 3 Sub-analysis of αβ+DNT cell numbers according to the main drug regimensFurthermore, no correlations were observed between αβ+DNT cell count and inflammatory parameters (such as ESR), or the disease activity index (JADAS-10) in JIA patients. In pSLE patients, we observed a trend of a moderate positive covariation of αβ+DNT cells with ESR when expressed as percentages of total lymphocytes or T cells (r = 0.525, P = 0.081; and r = 0.554, P = 0.065, respectively). Conversely, when αβ+DNT cells were expressed as an absolute cell count, they showed a trend of a negative correlation with pediatric SLE Disease Activity Index (pSLEDAI), though this did not reach statistical significance either (r = − 0.523, P = 0.479), likely due to the small sample size. We also considered disease duration as an additional parameter related to disease stage, but did not find a correlation with the number of αβ+DNT cells. This covariation analysis is graphically summarized in Fig. 3c.
Analysis of αβ+ double-negative T cells according to patients’ ageAs mentioned earlier, rheumatic children and controls differ in age in this preliminary study. Therefore, to assess whether this age disparity may have impacted the significant difference in αβ+DNT cells number overall, we performed a sub-analysis within two main age groups: study participants aged 2–9 years (group 1) and those aged 10–17 years (group 2). This approach enabled us to compare rheumatic children and controls without any significant age differences within each group. Significant difference in the number of circulating αβ+DNT was found between children with rheumatic diseases and normal controls, which remained consistent in both age groups, regardless of the method used to count these cells (Table 4).
Table 4 Analysis of αβ+DNT cells and main parental populations according to the patients’ ageThis analysis further supports a real difference in the circulating αβ+DNT cell pool, despite the age difference between rheumatic patients and controls in the whole study population. Moreover, the comparison between groups 1 (younger children) and 2 (older children) in either rheumatic patients or controls did not show any differences in the circulating pool of αβ+DNT cells according to age (Supplementary Table 3), which further indicates no significant age-dependent variations of these cells. Finally, the linear regression analysis also supports this statement. Although a slight inverse relationship between age and αβ+DNT cell number was present in rheumatic patients (Supplementary Fig. 1), it was not pronounced enough to imply any analytical bias related to the age of the study participants. Moreover, these subtle age-related trends of αβ+DNT cells are likely attributable to the higher general lymphocyte counts in younger children within our study population (Table 4 and Supplementary Table 3), as it is also established in the pediatric age-related reference ranges for lymphocyte number, regardless of ethnicity [10,11,12].
Therefore, taken together, all these observations and analyses confirm the existence of a statistically significant increase in αβ+DNT cells in the bloodstream of children with rheumatic diseases, which is not attributable to the age difference between these groups.
留言 (0)