
記住我


A cohort of 110 patients with ankle fractures who underwent surgery were analysed; 99 (90.0%) had lateral malleolus involvement (Table 1). Of these patients, 97 met the inclusion criteria, including 40 males (41.2%) and 57 females (58.8%). They ranged from the young to older individuals, averaging 49.6 years (age range: 17–89 years). The main injury mechanisms were low-energy injuries (89.7%). Using the Danis–Weber and Lauge–Hansen classification systems (Table 2), 83 fractures were classified as trimalleolar (85.6%) and 14 were classified as lateral and posterior malleolar fractures (14.4%). The Danis–Weber classification identified type B as the most common (83.5%), followed by types C (15.5%) and A (1.0%). The Lauge–Hansen classification showed posterior external and anterior external rotations in 82 and 10 cases (83.5 and 10.3%), respectively, and others less frequently. There was a strong correlation between the Danis–Weber and Lauge–Hansen classification systems, consistent with the findings of previous studies [24, 25].
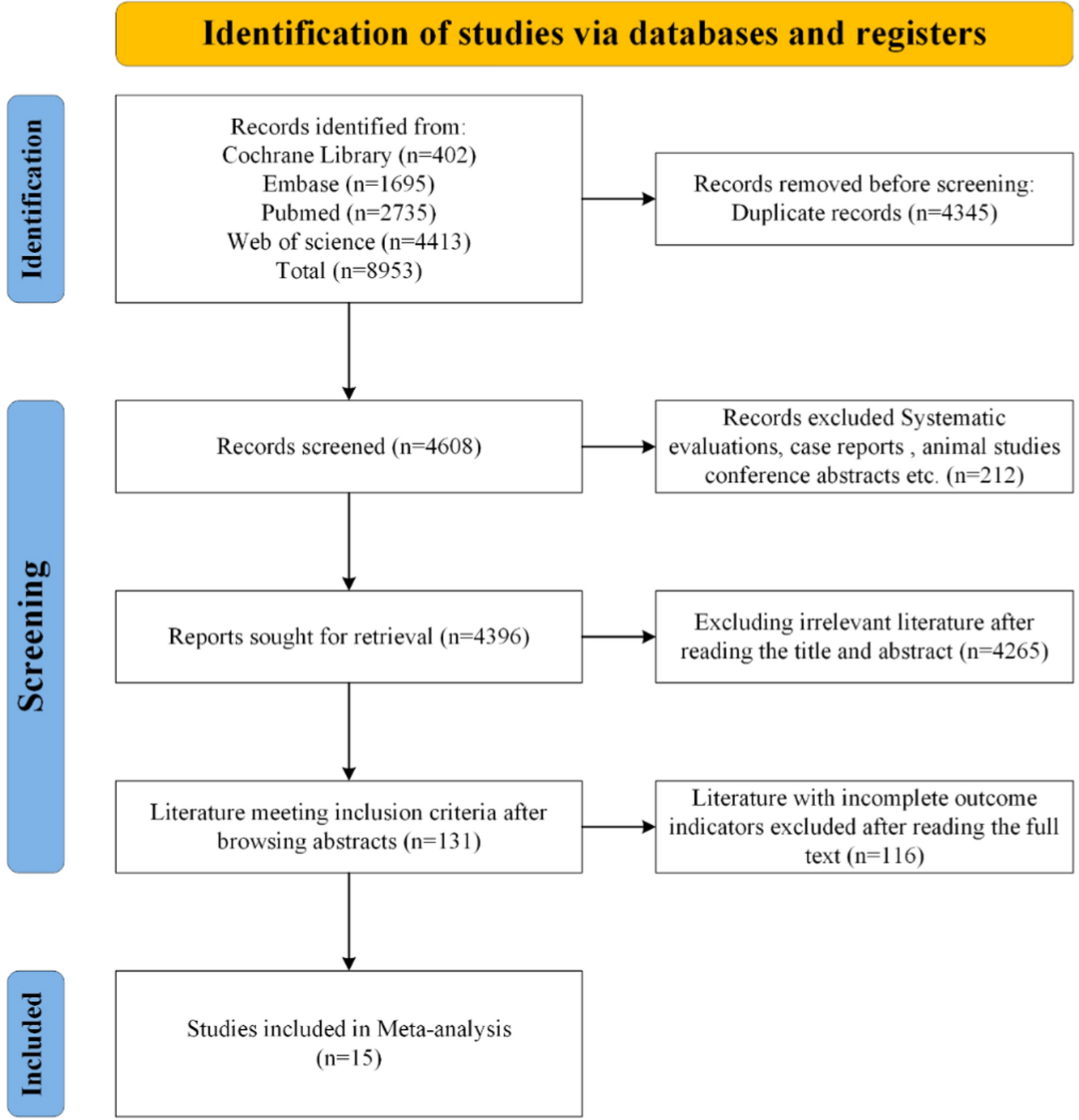
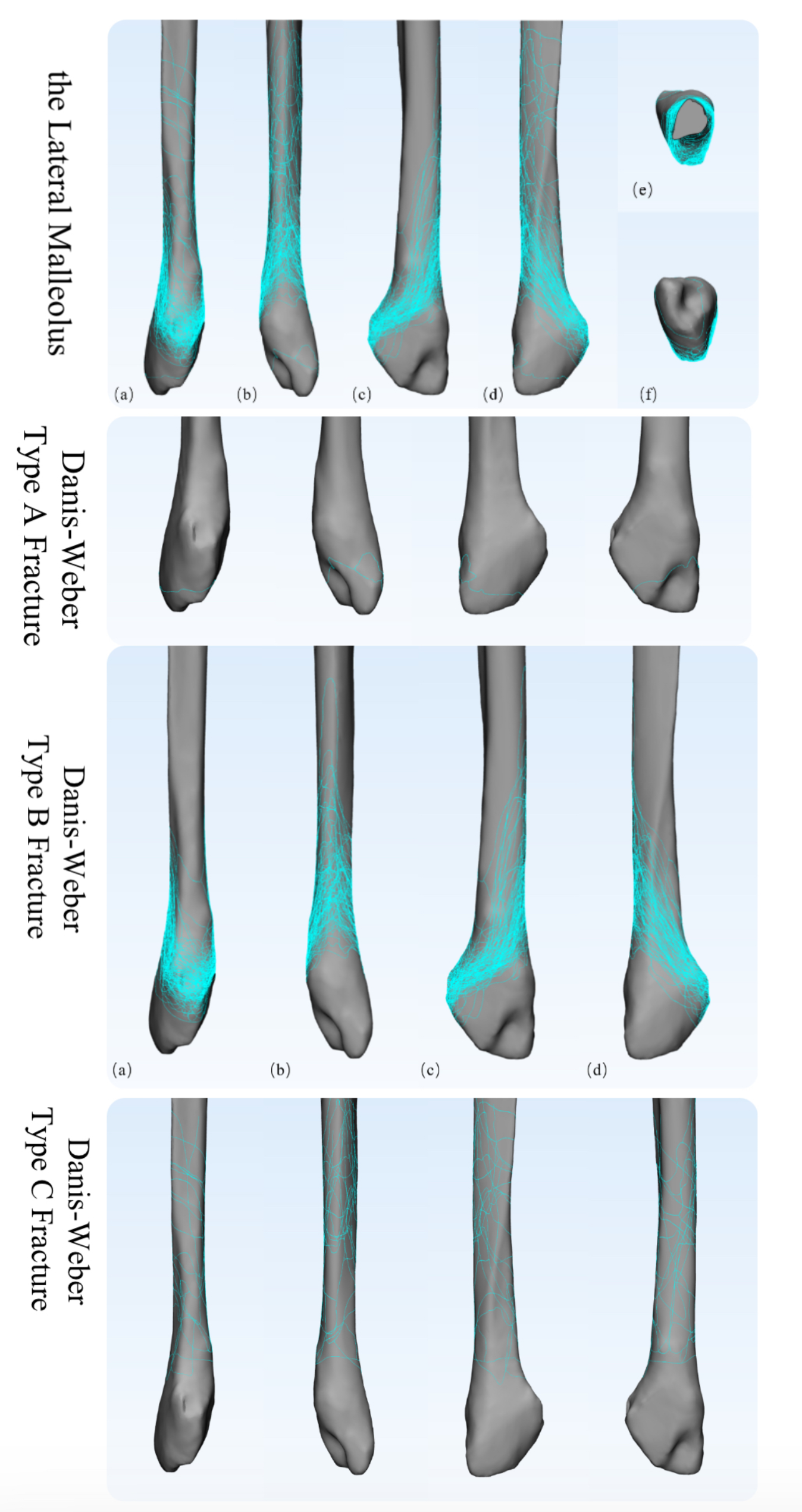
Table 1 Demographic characteristics of patients with ankle fracturesTable 2 Fracture types of fibula fracture patientsLateral malleolus fracture mapsFigure 1 shows the 3D lateral malleolus fracture map from 97 patients, layering all fracture lines on a standard model. Fractures at the distal tibiofibular syndesmosis, typical of Danis–Weber type B fractures, were the most frequent and ran obliquely. Type C fractures above the syndesmosis were followed, with lines categorised using the Danis–Weber system.
Fig. 1
Three-dimensional fracture maps
(a) Anterior view; (b) Posterior view; (c) Medial view; (d) Lateral view
The singular type A fracture observed in this study showed a fracture line encircling the tip of the lateral malleolus below the syndesmotic plane.
In Danis–Weber type B fractures, the line is located at the distal tibiofibular syndesmosis (Fig. 1). The map illustrates these fractures as concentrated antero-inferiorly in the fibula, starting from the Wagstaffe-Le Fort tubercle and obliquely extending posteriorly and superiorly to the posterior edge of the fibula, forming a low-anterior, high-posterior oblique ellipse. The oblique fracture line was symmetrically distributed in the medial and lateral views, with a more pronounced slope in the medial view. The oblique line angle varied widely, from 33.5° to 74.3° (average, 49.2°). The dense areas on the fracture map confirmed type B fracture as the most common lateral malleolus fracture, with no further classification. In some cases, additional fragments beside the mainline indicated further refinement of the fracture classification.
Type C fractures showed scattered lines above the syndesmosis concentrated posteriorly in the fibula, indicating possible comminution. The fracture map lacked a clear pattern with variable line heights and inclinations.
Morphological classification description based on the mapDanis–Weber type B fractures, which are oblique, are the most prevalent fractures based on the position of the fracture line relative to the distal tibiofibular syndesmosis. Significant findings were observed in the construction of the fracture maps for these 81 cases.
Only 33.3% (27 cases) of the fractures showed an oblique fracture line in the two parts.
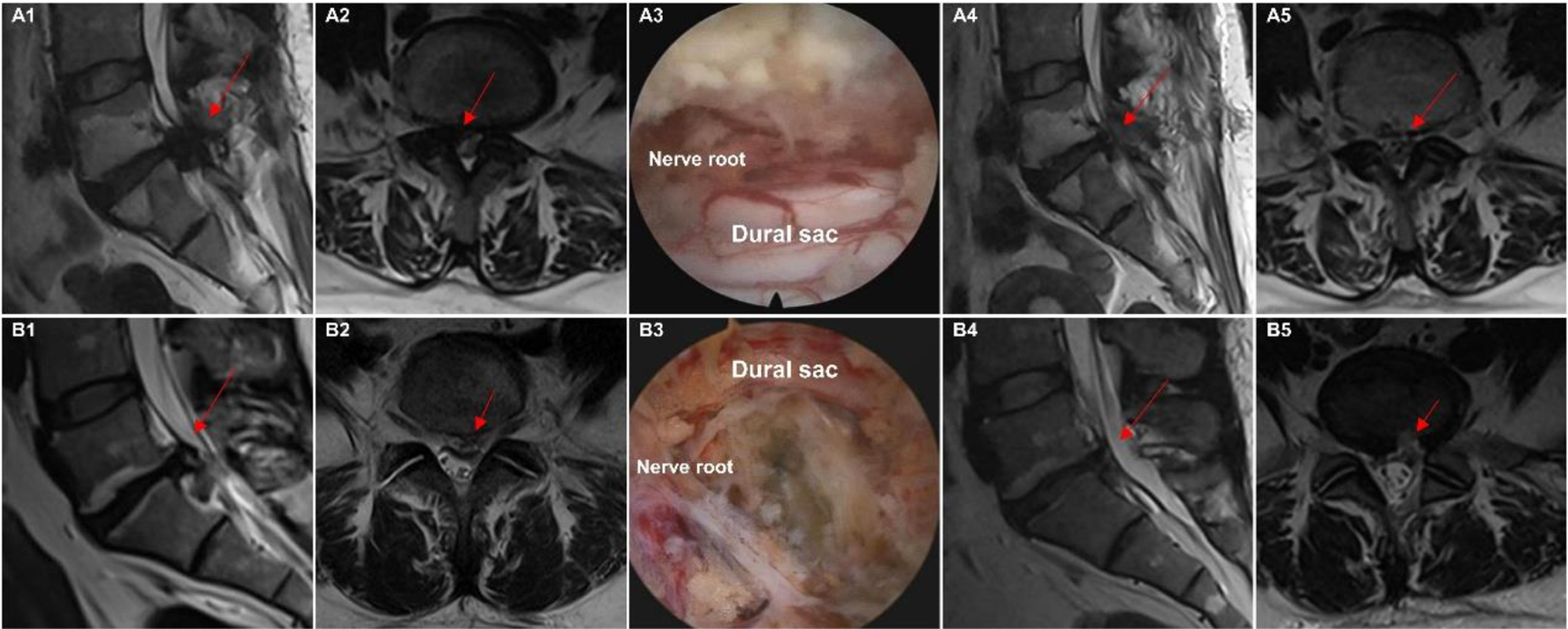
Among 58.0% of type B fractures, an additional anteroinferior fragment was found in 47 cases (single or comminuted), averaging 11.9 mm in length [26,27,28]. These triangular or diamond-shaped fragments, indicative of anterior inferior tibiofibular ligament (AITFL) avulsion, were more frequently identified in our 3D analysis than in 1.5–26.5% of cases. Figure 2 illustrates a typical case showing the location of the fragment on CT. These fragments often appear uplifted post-3D modelling and are potentially overlooked on standard CTs. As shown in Fig. 2, the mapped fracture lines confirmed fragment avulsion from the AITFL at the Wagstaffe-Le Fort tubercle.
Fig. 2
Anteroinferior bone fragment (A).Typical case with an anteroinferior bone fragment (a-c) Three-dimensional CT images of the patient, with arrows indicating the bone fragment; (d) After modeling, only the main proximal and distal parts of the fracture are reduced, with the arrow indicating the uplifted AITFL avulsion bone fragment; (e-h) Model after completion of bone fragment reduction, with anterior, posterior, medial, and lateral views.(B) Distribution map of the anteroinferior bone fragment (a) Anterior view; (b) Medial view; (c) Lateral view
Posterosuperior fragments were identified in 19.8% (16 cases) of fractures, with sizes of 3.5–32.7 mm, averaging 14.6 mm in length, and typically strip-shaped. Figure 3 shows a typical case of fragment marking in the pre-reduction images. Figure 3’s distribution map illustrates their locations, and Table 3 presents the characteristics of posterosuperior and anteroinferior fragments.
Fig. 3
Posterosuperior bone fragment
(A) Typical case with a posterosuperior bone fragment(a-c) Three-dimensional CT images of the patient, with the bone fragment indicated by the arrow; (d) Modeling after only the main proximal and distal parts of the fracture are reduced, with the bone fragment indicated by the arrow; (e-h) Model after the bone fragment is completely reduced, with anterior, posterior, medial, and lateral views;
(B) Distribution map of the posterosuperior bone fragment (a) Posterior view; (b) Medial view; (c) Lateral view
Table 3 Description of accessory bone fragments associated with main fracture linesDanis–Weber type B fractures at the distal tibiofibular syndesmosis were further classified based on the presence of two bone fragment types into the following: type i, simple oblique fracture; type ii, anteroinferior fragment without a posterosuperior fragment; type iii, posterosuperior fragment without an anteroinferior fragment; and type iv, both fragments present.
Clinical research resultsFollowing fracture map creation, we clinically analysed lateral malleolar fractures and proposed a classification system to assess the severity of ankle joint injury, distal tibiofibular stability, and prognosis.
Severity of ankle joint injuryBy analysing Danis–Weber type B fractures using the fracture map, we noted additional fragments in types i–iv and their impact on ankle injury severity, as shown in Table 4. Statistically, the presence of fragments (types ii + iii + iv) correlated with a higher rate of severe injuries than in the simple fracture group (type i), with a P-value < 0.05.
Table 4 Comparison of injury severity between B-type fractures with and without bone fragmentsIntraoperative stability of the distal tibiofibular syndesmosisTo determine the necessity of fixation, we intraoperatively evaluated distal tibiofibular syndesmosis stability in patients with lateral malleolus fractures through stress testing and radiography. Additional file 1 presents the stability comparison between Danis–Weber types B and C, with type C showing significantly lower stability, consistent with the findings in previous studies [14].
Our improved classification of Danis–Weber type B fractures showed no significant difference in stability between the groups with (types ii, iii, and iv) and without bone fragments (type i). Further analysis of the impact of the anterior inferior and posterior superior fragments on syndesmotic stability revealed no significant differences in the stability rates among the affected groups.
In Danis–Weber type B fractures, an anteroinferior AITFL avulsion bone fragment or a posterior superior fragment does not affect distal tibiofibular syndesmotic stability significantly.
Follow-up results and prognosis analysisIn this study, 81 of 97 patients with lateral malleolus fractures completed a minimum of a 4-year follow-up, contributing to clinical scores and radiographic assessments. One type A case was lost, and 67 and 14 type B and C cases, respectively, were analysed. The refined classification included 22 B-i, 34 B-ii, 5 B-iii, and 6 B-iv cases, and one B-i case had a wound infection. An additional table file presents the prognostic scores (the AOFAS, OMAS, VAS, and patient satisfaction scores) and K-L grades [see Additional file 2].
The prognostic differences in type B fractures were investigated by comparing those with additional bone fragments (ii + iii + iv, 45 cases) with those without (type i, 22 cases). An additional table file shows that the group with fragments had lower mean AOFAS and OMAS scores and a higher mean K-L grade, although the differences were not significant (P > 0.05, Mann–Whitney U test) [see Additional file 3].
Further analysis of the anterolateral and posterolateral bone fragments [see Additional files 4 and 5] revealed no significant prognostic score differences. An additional table file shows that the Spearman’s test revealed no significant association between the anterolateral bone fragment size and prognosis scores (P > 0.05).
留言 (0)