
記住我
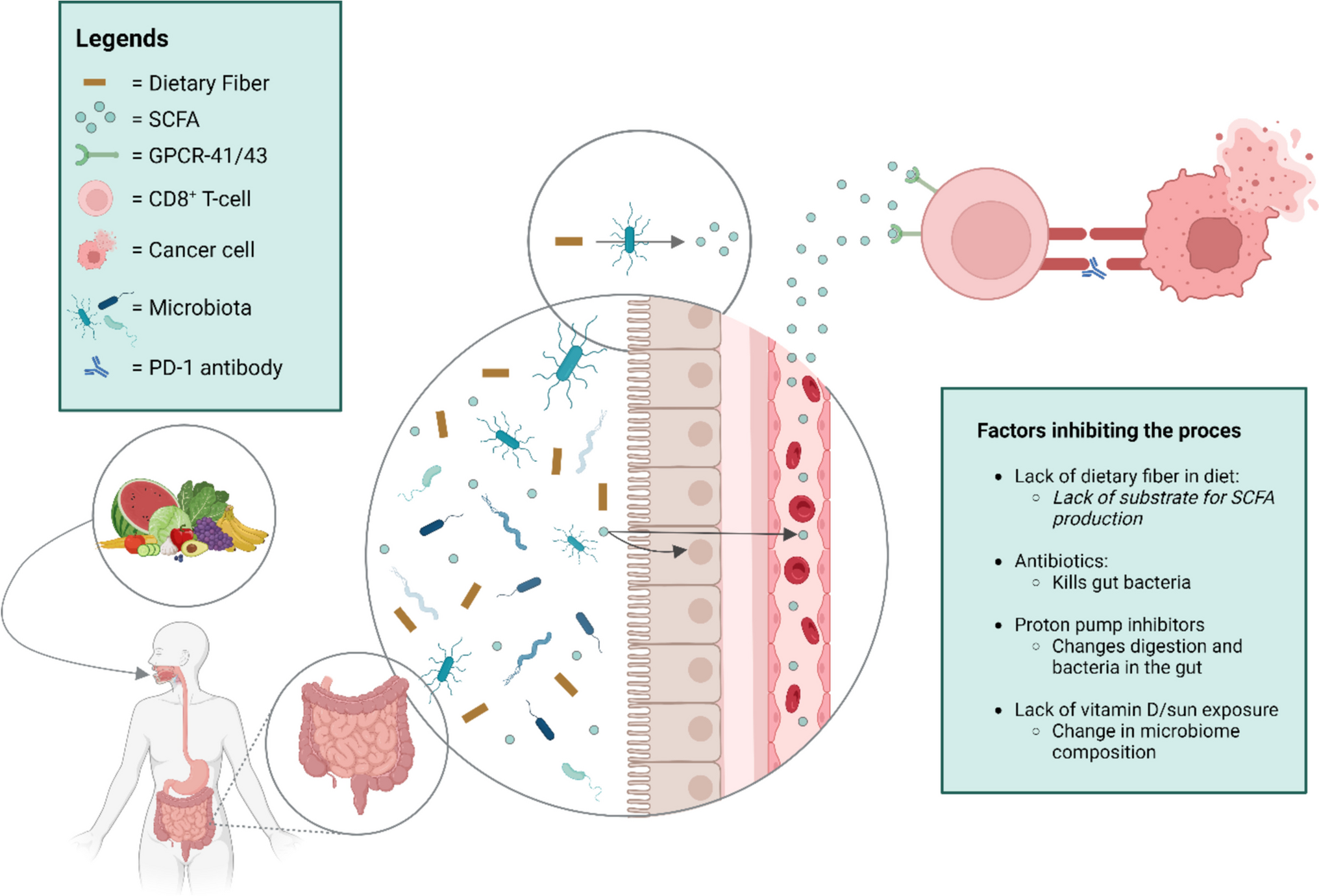


The metabolome consists of the molecules produced by gut bacteria. Among these are short-chain fatty acids (SCFAs), which are small molecules produced by the gut commensal microbiome when fermenting dietary fiber and phytochemicals. The most common SCFAs are acetate, propionate, and butyrate. SCFAs are important as an energy source for intestinal epithelial cells, but some also enter the bloodstream and act as signaling molecules. They target G-protein-coupled receptors (GPCR) GPCR41, GPCR43, and GPCR109A [53] (Fig. 1). Recently, Zhu et al. demonstrated a positive correlation between serum butyrate levels and response to anti-PD-1 immunotherapy in patients with NSCLC [50].
Fig. 1
Following the consumption of a high-fiber diet, bacteria in the gut ferment dietary fiber to short-chain fatty acids (SCFAs). Some of the SCFAs nurture intestinal epithelial cells, and some enter the bloodstream. Here SCFAs can activate DC8 + cytotoxic T-cells to induce cancer cell death by binding to mammalian G protein-coupled receptors (GPCR) 41 and 43. This unique ligand specificity suggests that GPCR41 and GPCR43 may mediate the interaction between the gut microbiome and the human host
Factors that may Positively Impact the Microbiome for Response to ICI TherapyUnderstanding that the microbiome impacts the effectiveness of cancer immunotherapy, how can we influence it to improve treatment outcomes? And what should we avoid to reduce its efficacy?
Dietary fiber and ProbioticsDietary fiber is plant material that human gut enzymes cannot digest [54] but can be fermented by gut bacteria. Spencer et al. studied whether dietary intake of prebiotic fiber and probiotics affect treatment response to checkpoint immunotherapy in melanoma patients. They found that patients consuming more than 20 g of dietary fiber daily before treatment had significantly longer progression-free survival than those consuming less than 20 g. For every 5 g of fiber intake, there was a 30% decrease in the risk of progression or death [28]. Interestingly, the intake of probiotics did not alter PFS or the odds of response to checkpoint immunotherapy in patients with low fiber intake. In patients with high fiber intake, the addition of probiotics had a detrimental effect on the response to treatment, similar to patients with low fiber intake [28].
Even an intake of 20 g of dietary fiber daily, met by only one-third of patients [28], is low compared to recommendations. US guidelines recommend 14 g per 1000 calories consumed, and Nordic guidelines recommend 25–35 g daily depending on calorie intake. These recommendations are based on amounts to prevent constipation or cardiovascular disease, not on current knowledge regarding the requirements of the gut microbiota. Increasing the recommendation to 50 g daily should meet the requirements of the microbiota, but this is 2–3 times the amount consumed today by an average Western person. Achieving this will require extensive education of healthcare professionals and the public [54, 55].
Pietrzak et al. surveyed various factors, including food and medicine intake, in Polish melanoma patients [39]. Certain types of bacteria were related to response to anti-PD-1 therapy and the patient’s diet was important. They examined 35 different factors and discovered that consumption of plant foods was positively correlated with a better response to anti-PD-1 treatment, while dairy consumption had the opposite effect.
Additionally, they observed that patients who defecated daily responded better than patients defecating every other day [39]. This could be related to higher plant fiber intake. An unexplained difference in response was found in patients with Rh+/- blood types, which will require further investigation [39]. All other factors investigated did not show significant differences between responders and non-responders [39].
The American Gut project investigated how diet influences gut bacteria diversity by collecting microbiome samples from over 10,000 people. Samples were correlated with lifestyle, health, and disease questionnaires. They compared the microbiomes of people consuming fewer than 10 different plants weekly with those consuming more than 30 different plants weekly. The results showed that the microbiomes of high plant consumers were significantly more diverse. This finding aligns with current knowledge that different strains of bacteria metabolize different types of plant materials, so a more varied plant diet supports a wider variety of bacteria [56].
Mediterranean dietThe Mediterranean diet consists of ingredients native to the countries around the Mediterranean Sea. It includes a variety of plant foods such as vegetables, fruits, nuts, seeds, berries, legumes, herbs, and spices. It also features animal proteins like fish, meat, cheese, and other fermented dairy products from locally raised animals, along with fat from olive oil. This traditional diet also incorporates ancient grains, honey, and wine [57]. These foods provide a naturally high intake of dietary fibers with various molecular structures and different phytochemicals from many types of plants, supporting a wide range of gut bacteria. Two trials in melanoma patients by Spencer et al. [28] and Pietrzak et al. [39]. indicated that a high intake of plant foods and dietary fiber was positively correlated with a better response to immunotherapy. These findings suggest that the Mediterranean diet could improve response rates to immunotherapy. However, more clinical trials are needed to confirm this, especially in patients with other types of cancer and those undergoing combination treatments.
Sun exposure/vitamin DVitamin D is unique because it is mostly supplied by sunlight rather than diet. A recent study on cancer patients and mice explored the link between vitamin D, the microbiome, and response to immunotherapy. The data suggested that lower vitamin D availability is associated with weaker immune-mediated control and worse cancer outcomes [58]. In a cohort of almost 1.5 million Danes who had at least one measurement of vitamin D status in 2008–2017, 1008 persons were recorded as having been treated with immunotherapy for various cancers. In this group, vitamin D/vitamin D receptor levels were significantly lower (p ˂ 0.0001) in patients who had no response to immunotherapy versus those with exceptional response to immunotherapy. When studying the rate of progression they also found that patients with low levels of vitamin D/ vitamin D receptor levels more often had a rapid progression versus those with standard disease progression (p = 0.02). This part of the study did unfortunately not correlate outcomes to the microbiome [58].
In a study of melanoma patients, sufficient vitamin D levels during immunotherapy treatment were correlated with better ORR and PFS. The response rate in the group with low vitamin D levels and not supplemented versus normal baseline levels or a normal level obtained with supplementation was 36.2%, versus 56.0% (p = 0.01); progression-free survival was 5.75 and 11.25 months, respectively (p = 0.03). Unfortunately, this trial did not investigate the effect on the microbiome [59].
In cancer patients, the direct impact of sun exposure on the microbiome has not been studied. However, a study involving healthy female volunteers from Vancouver, Canada, found that exposure to artificial ultraviolet-B (UVB) light during winter increased serum vitamin D levels and altered the gut microbiome in participants not taking vitamin D supplements. Bacteria like Lachnospiraceae and Ruminococcus, which positively impact immunotherapy response, were low in patients not taking vitamin D supplements but increased after UVB exposure. Additionally, both alpha and beta diversity of the microbiome increased after UVB exposure [60].
Vitamin D levels are generally low in many parts of the world, especially during winter. Supplementing with vitamin D can help compensate for the lack of sun exposure [60].
Factors that may Negatively Impact the Microbiome in Response to ICI TherapyPharmacomicrobiomics is the science of interactions between medicines and the microbiome. While these interactions can be bidirectional, this review focuses on how medicines commonly prescribed to cancer patients, other than cancer drugs themselves, can affect the microbiome.
A single-center retrospective study involving 635 cancer patients treated with immunotherapy investigated whether different co-medications affected their response to treatment, either as single agents or in combination. They found that antibiotics, proton pump inhibitors (PPIs), and corticosteroids (at doses over 10 mg), taken one month before or after starting immunotherapy, had a detrimental effect on immunotherapy efficacy. This was also true for morphine and psychotropic medicines. However, other commonly prescribed medicines such as metformin, other oral anti-diabetic medicines, ACE inhibitors, angiotensin II antagonists, statins, and aspirin did not show the same negative effect. The data were not correlated with microbiome measurements, so it is unclear whether these effects are due to changes in the microbiome or other mechanisms [61].
AntibioticsSeveral investigators have found that using antibiotics during or just before starting PD-1 immunotherapy leads to worse outcomes compared to patients not treated with antibiotics (Fig. 2). Routy et al. discovered that the composition of the gut microbiome was crucial and that antibiotics around the time of starting immune checkpoint inhibitors in patients with NSCLC or RCC reduced the response to therapy [20]. Spencer et al. found similar results in melanoma patients, even those on a high-fiber diet [28]. In a study of 69 NSCLC patients Hamada et al. found that those who received antibiotics 21 days before or after starting anti-PD-1 treatment (N = 18) had significantly worse outcomes than those not treated with antibiotics (N = 51); overall response rate (p = 0.005), OS (p = 0.022) and PFS (p ˂ 0.001) were all negatively affected [62]. The study also showed that antibiotics given more than 21 days after starting anti-PD-1 treatment did not affect treatment efficacy [62].
Proton pump InhibitorsCantarelli et al. examined the impact of proton pump inhibitors (PPI) on cancer patients undergoing immunotherapy. In a single-center retrospective cohort of 302 patients, more than 75% used PPIs either before or during cancer therapy. They found that PFS and OS were significantly lower in the PPI-treated group (Fig. 2) [63]. The study suggested a treatment window where starting PPIs four weeks after initiating immunotherapy might mitigate their negative effects [63]. Similar results were observed in a study of advanced NSCLC patients where PPI use was associated with lower PFS and OS. However, adding Clostridium butyricum to the treatment regimen reversed the negative effect of PPI usage [64]. Not all studies show the same results. For instance, a study by Peng et al. on 233 cancer patients found no difference between PPI users and non-PPI users [65], and the same was true for Hamada´s study on 69 patients with NSCLC [62]. To clarify the impact of PPIs, Lopes et al. conducted a meta-analysis of 41 studies including 20,042 patients. They concluded that PPI use negatively affects both OS and PFS in patients receiving immunotherapy [66].
Discussion/Feasibility of Mediterranean diet in real-world PatientsIt can be challenging to make diet and lifestyle changes when a patient is stressed due to a new diagnosis or relapse. However, many patients want to improve their lifestyle. A systematic review by Hoedjes et al. of 30 studies on dietary changes in cancer patients, revealed that support from family, friends, and healthcare professionals was a key factor in making changes. Barriers included not understanding the importance of dietary changes and not receiving information and advice from healthcare professionals (Fig. 2). Patients saw lifestyle changes as a positive way to gain control [67].
In a recent review of the implementation of Mediterranean-style dietary intervention in cancer patients, McHugh et al.. investigated the methods, feasibility, and primary efficacy of such interventions [68]. The studies used dieticians or other hospital personnel to educate patients in the intervention groups. In 11 of 13 studies, the completion rates were 80% or higher. In four of five clinical trials, with patients on active cancer treatment during the intervention the completion rate was 80% or higher. These results indicate that dietary interventions are feasible for patients undergoing cancer treatment [68].
The Mediterranean diet includes a wide variety of foods, making it a flexible option for many patients. It is not restrictive, and primarily limit processed foods. This flexibility was a key reason why Harvey et al. chose this diet for a randomized clinical trial involving cancer patients. The study measured fatigue during chemotherapy and included a qualitative sub-study, identifying facilitators and barriers [69]. Patients reported that the diet gave them a sense of control and empowerment. They enjoyed learning about nutrition, trying new foods, feeling in control, setting goals, doing something constructive to aid their treatment, and having a positive focus. Even patients in the control group started thinking more about their eating habits. Barriers included chemotherapy side effects and food preferences [69].
These findings indicate that patients are motivated to change their diet, and encouragement from their healthcare team can be a significant motivating factor.
Fig. 2
Right panel Summary of factors with strong evidence for positively or negatively affecting immunotherapy treatment outcomes through the microbiome. Left panel Factors that help or hinder dietary changes during cancer treatment
Future PerspectiveWhat can we expect from the future? It seems that the microbiome plays a role in cancer immunotherapy, and the mechanisms behind are being uncovered. It appears that the microbiome can be used as a predictive marker of response. To maximize the efficacy of immunotherapy and to possibly benefit more patients, it will be necessary to test whether manipulating the microbiome composition can increase response rates.
留言 (0)