ESO-Shanghai 13
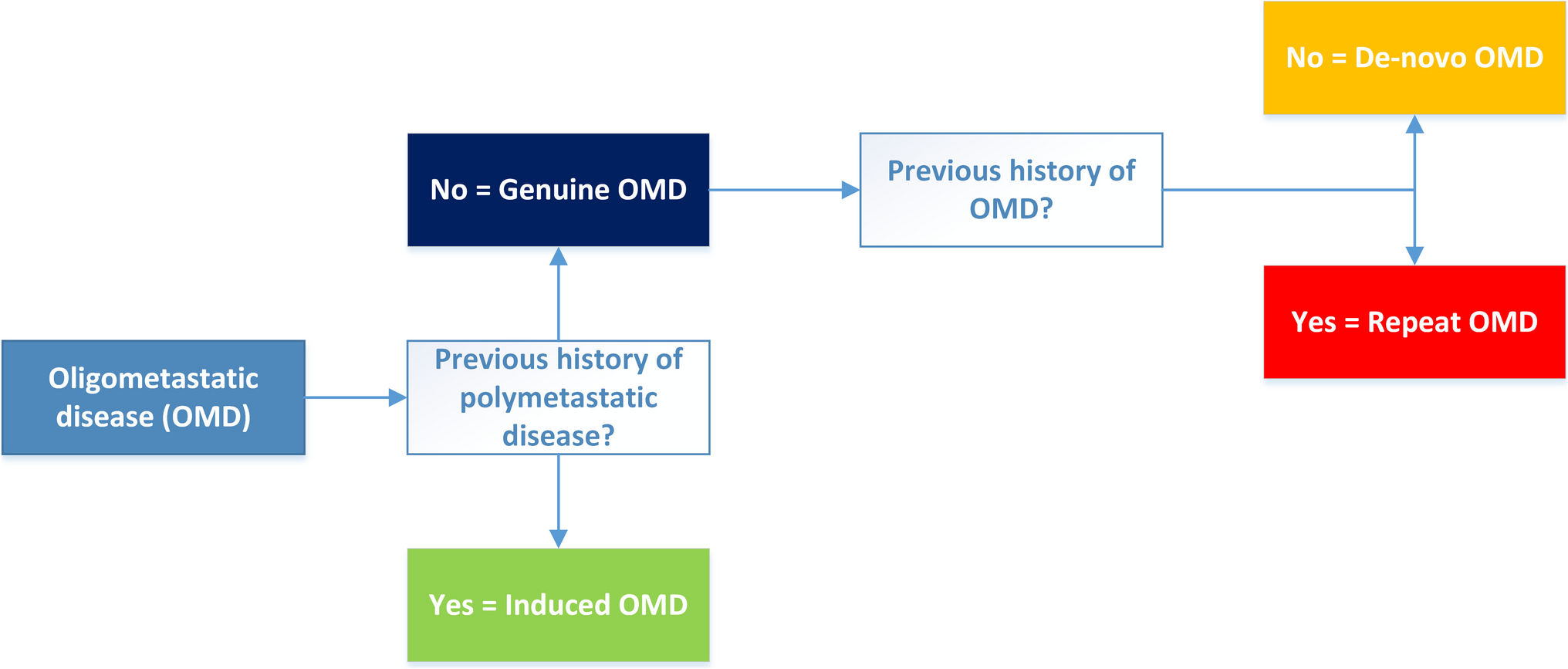
In the Chinese phase II ESO-Shanghai 13 trial, 116 patients over 18 years old with an ECOG performance status of 0–1 and confirmed metachronous oligometastatic squamous cell carcinoma of the esophagus were enrolled between March 2019 and September 2021 [16]. Patients had a controlled primary tumor through surgery or radiotherapy with no progression for at least 3 months [16]. De-novo OMD was characterized as having ≤ 4 metastatic sites in ≤ 3 different organs, each lesion measuring ≤ 5 cm, and all being suitable for local treatment without previous intervention [16]. Patients who had received antitumor treatments within the last 3 months or had polymetastatic disease were excluded from the trial [16].
The study randomized 104 patients 1:1 to receive either standard-of-care systemic therapy alone or combined systemic and local therapy. Randomization was balanced on 3 prognostic factors: number of disease sites (1 vs. 2–4), prior systemic therapies (first-line vs. second-line), and metastases location (non-regional lymph nodes vs. visceral metastases) [16]. Both groups underwent 4 cycles of standard chemotherapy, with an option for anti-PD-1 immunotherapy starting July 2020 [16]. The local therapy group, which included 20 of 53 patients receiving immunotherapy, had radiotherapy as the preferred treatment of choice, using stereotactic ablative body radiotherapy (SABR) in 38%, intensity-modulated (conventional) radiotherapy in 47%, and hypofractionated radiotherapy in 4% [16] SABR often entailed ≤ 5 fractions of ≥ 7 Gy, while conventional radiotherapy used ≥ 45–66 Gy at 1.8–2.0 Gy per fraction [16]. Other local treatments included surgery or thermal ablation [16]. In the systemic therapy group, local treatments were restricted to cases of disease progression, symptom relief, or palliative care [16].
The primary study endpoint was progression-free surviva, with secondary endpoints including overall survival, local control, toxicity, and quality of life [16]. The study showed a significant survival benefit for the group receiving combined therapy, with a median progression-free survival of 15.3 months compared to 6.4 months in the systemic-only group (stratified hazard ratio [HR] 0.26, 95% CI 0 16–0.42; p < 0.0001) [16]. This improvement in progression-free survival also led to an improved overall survival, where the median overall survival was not reached in the combined therapy group versus 18.6 months in the systemic therapy-only group (HR 0.42, 95% CI 0.24–0.74; p = 0.002) [16]. Notably, the addition of local therapy seemed less beneficial for patients receiving immunotherapy (HR for progression-free survival 0.49 [0.24–0.99]; log-rank p = 0·044 and HR for overall survival 0.57 [95% CI 0.24–1·36]; p = 0.19) [16]. The pattern of treatment failure also varied, with a higher occurrence of new lesions in the combined therapy group but significantly better local control (HR 0.11, 95% CI 0.05–0.24; p < 0.0001) [16]. The time until new lesions appeared was longer in the combined therapy group (16.8 months) compared to the systemic-only group (12.3 months; p = 0.0075) [16].
IKF-575/RENAISSANCE Phase III Trial
In the German IKF-575/RENAISSANCE phase III trial, presented at ASCO 2024, 182 patients aged at least 18 years, with an ECOG performance status of 0–1 and histologically confirmed synchronous de-novo OMD from adenocarcinoma of the stomach or gastroesophageal junction were included between February 2016 and May 2024 [17]. De-novo OMD was defined as retroperitoneal lymph node metastases only or/and peritoneal carcinomatosis, ≤ 5 liver metastases, unilateral lung involvement, uni- or bilateral ovarian metastases, uni- or bilateral adrenal gland metastases, extra-abdominal lymph node metastases, or localized bone involvement [17].
A total of 139 patients were randomized 1:1 to standard-of-care systemic therapy combined with local therapy for all metastases (Arm A) or systemic therapy alone (Arm B) [17]. Patients were balanced by three prognostic factors: primary tumor location (gastric cancer vs. gastroesophageal junction), response to systemic therapy (complete response/partial response vs. stable disease), and location of the metastases (retroperitoneal lymph node metastases only vs. visceral metastases) [17].
Systemic therapy for both groups consisted of 4 cycles of standard-of-care fluorouracil, leucovorin, oxaliplatin and docetaxel (FLOT) chemotherapy [17]. Post-randomization, patients without disease progression were randomized into two arms [17]. Arm A received surgery followed by 4–8 cycles of FLOT chemotherapy, while Arm B received 4–8 cycles of FLOT chemotherapy alone [17].
The primary endpoint of the study was overall survival, with secondary endpoints including the proportion of patients with local control, toxicity, and quality of life. Pre-specified subgroup analyses were performed for patients with (1) retroperitoneal lymph node metastases only, (2) liver metastases, and (3) peritoneal metastases [17].
Patients in both groups were well balanced in baseline characteristics, including performance status and TNM stage [17]. Both groups received a similar number of pre-randomization chemotherapy cycles [17]. Surgery was performed in 91% of patients in Arm A, but also in 21% of patients in Arm B. In Arm A, complete resection of both the primary tumor and metastases was achieved in 56% of patients with retroperitoneal node metastases and 53% of patients with visceral metastases [17]. However, there was a difference in the number of received cycles of post-randomization chemotherapy) [17].
The study demonstrated that the cohort receiving systemic and local therapy (Arm A) had comparable overall survival to the systemic therapy-only cohort (Arm B) [17]. Median overall survival was 18.5 months (interquartile range [IQR]: 9.5–65.2) in Arm A versus 23.6 months (IQR: 14.0–41.2) in Arm B (p = 0.861) [17]. A benefit of additional local therapy was observed in patients with retroperitoneal lymph node metastases only, with a median overall survival of 29.6 months versus 17.1 months (Arm A compared with Arm B) [17]. Patients with liver metastases had comparable overall survival (24.9 versus 25.7 months), while those with peritoneal metastases had worse overall survival in Arm A compared to Arm B (11.9 vs. 18.6 months) [17]. After the end of study treatment, there was a difference in proportion of patients receiving further anticancer therapy (52% in arm A versus 82% in arm B) [17].
In summary, ESO-Shanghai 13 and RENAISSANCE report conflicting results on the benefit of local treatment for de-novo OMD. These conflicting results can be explained by several key differences between the studies [16]. Firstly, the primary tumor type and histology: the ESO-Shanghai study [16] included only patients with esophageal squamous cell carcinoma, whereas the IKF-575/RENAISSANCE trial [17] included patients with gastric or gastroesophageal junction adenocarcinoma. Secondly, the type of OMD: the ESO-Shanghai study included patients with metachronous de-novo OMD, had a lower cut-off for the number of metastases (4) and did not include patients with peritoneal metastases, whereas the IKF-575/RENAISSANCE trial included patients with synchronous de-novo OMD, had a higher cut-off for the number of metastases (5) and included patients with peritoneal metastases [16, 17]. Thirdly, the treatment of OMD: the ESO-Shanghai study predominantly used radiotherapy (SABR), [16] while the IKF-575/RENAISSANCE trial [17] used surgery for the primary tumor and metastases. In addition, it is important to note that a complete resection of the primary tumor and metastases was achieved in 56% of patients with retroperitoneal node metastases only and 53% of patients with visceral metastases in the IKF-575/RENAISSANCE trial [17].



留言 (0)