
記住我



Participant characteristics are shown in Table 1. Of the 92 respondents, the median age was 29 (range 25–46). The majority of respondents were White (n = 59, 58.4%), followed by Asian (n = 24, 23.8%). Respondents primarily identified as cisgender female (n = 49, 53.3%), followed by cisgender male (n = 41, 44.6%). Most respondents identified as heterosexual (n = 82, 89.1%). Additionally, few reported receiving training on EDs in their residency program (n = 19, 20.7%).
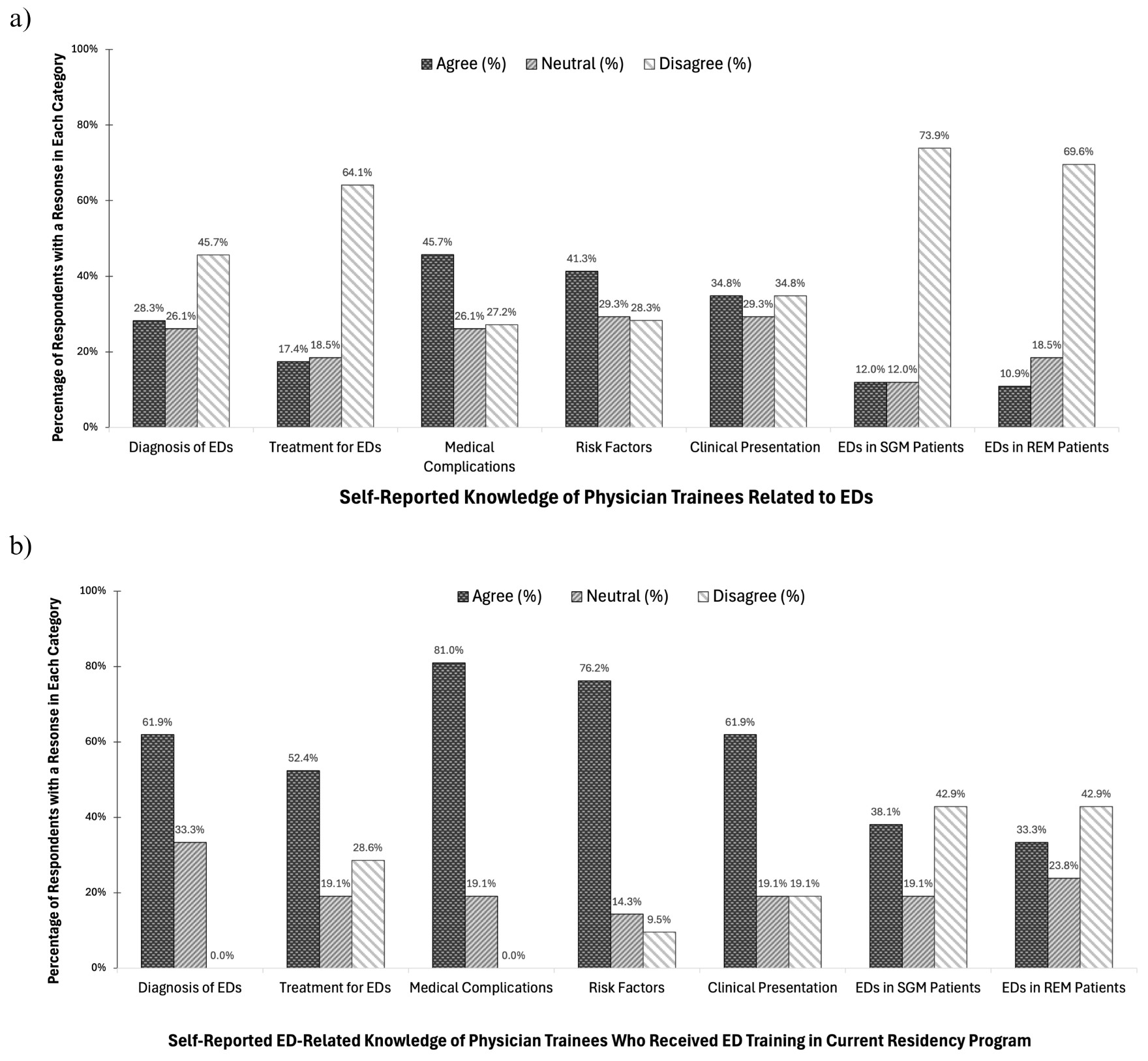
Table 1 Characteristics of study participantsKnowledge of eating disorder medical managementFigure 1a illustrates notable findings, including low self-confidence with regards to the diagnosis (n = 26, 28%) and treatment (n = 16, 17.4%) of EDs. Self-reported confidence in general eating disorder knowledge was highest for medical complications (n = 42, 45%), followed by risk factors (n = 38, 41%), and their clinical presentations (n = 32, 35%). Reported confidence in knowledge of EDs in diverse populations was much lower. Most respondents reported a lack of knowledge with regard to EDs in sexual and gender minoritized patients (n = 68, 73.9%) and in racial and ethnic minoritized patients (n = 64, 69.6%).
Figure 1b indicates that among respondents who received ED training at their current residency program (n = 21, 22.8%), most reported confidence with regards to the diagnosis (n = 13, 61.9%) and treatment (n = 11, 52.4%) of ED. Confidence was highest with regard to their knowledge of the medical complications (n = 17, 81%), risk factors (n = 16, 76.2%), and clinical presentations (n = 13, 62%) associated with EDs, respectively. Moreover, even among participants who received ED training at their current residency program, only a minority reported confidence in their knowledge of EDs in diverse populations, including sexual and gender minoritized patients (n = 8, 38.1%) and racial and ethnic minoritized patients (n = 7, 33.3%).
Fig. 1
a Self-reported knowledge of physician trainees related to EDs (n = 92). b Self-reported ED-related knowledge of the subset of physician trainees who received ED training in their current residency program (n = 21)
Table 2 indicates a relatively high level of knowledge regarding the medical management of EDs, captured by open-ended responses to vignette-style questions. For the acute management of EDs, respondents most frequently mentioned electrolyte monitoring with a basic or comprehensive metabolic panel (n = 81, 88.0%), psychiatric referral/evaluation (n = 44, 47.8%), complete blood count (n = 34, 37.0%), and screening/monitoring for refeeding syndrome with magnesium (n = 21, 22.8%) and phosphorus (n = 20, 21.7%). In addition, there is limited diversity in the perceptions of the characteristics of an ED patient (Table 2). Responses were predominantly associated with low body weight/BMI (n = 59, 64.1%), psychiatric comorbidities (n = 24, 26.1%), female gender (n = 19, 20.7%), and young (n = 13, 14.1%).
Table 2 Vignette-based assessment of knowledge of ED (a) management and (b) characteristics of EDsAttitudes and practices towards patients with eating disordersFigure 2a denotes that few respondents feel comfortable talking with patients about ED behaviors (n = 28, 30%). In addition, many indicated that they never (n = 34, 33%) or rarely (n = 37, 40%) take an ED history in their patients. Moreover, among racial and ethnic minoritized patients, several respondents reported they either never (n = 34, 37%) or rarely (n = 38, 41%) screen for EDs. Similarly, many indicated they never (n = 31, 34%) or rarely (n = 21, 23%) refer these patients to treatment. Comparable patterns were observed with sexual and gender minoritized patients, with many stating they never (n = 34, 37%) or rarely (n = 37, 40%) conduct screenings and most noting they never (n = 32, 35%) or rarely (n = 21, 23%) refer these patients with EDs to treatment.
Figure 2b indicates that most participants who received ED training at their current residency programs (n = 21, 22.8%) reported feeling comfortable talking to their patients about ED-related behaviors (n = 16, 76.2%). Additionally, few respondents who received ED training reported that they rarely (n = 8, 38%) or never (n = 0, 0%) take an ED history in their patients. In sexual and gender minoritized patients, few participants of this group indicated that they rarely (n = 7, 33.3%) or never (n = 0, 0%) screen for EDs. Likewise, few of these respondents indicated that they rarely (n = 3, 14.3%) or never (n = 2, 9.5%) refer these patients with EDs to treatment. In addition, among racial and ethnic minoritized patients, few respondents of this group indicated that they rarely (n = 8, 38.1%) or never (n = 0, 0%) screen for EDs. Similarly, a minority of respondents indicated that they rarely (n = 3, 14.3%) or never (n = 2, 9.5%) refer racial and ethnic minoritized patients with eating disorders to treatment.
Figure 2c shows that most respondents (n = 61, 66.3%) reported that they enjoy working with patients from sexual and gender minoritized backgrounds and would value further clinical training pertaining to the diagnosis and management of EDs in this population. Similarly, most respondents (n = 69, 75.0%) reported that they enjoyed working with patients from racial and ethnic minoritized backgrounds, and would value further clinical training with regards to EDs in this population. Lastly, few respondents reported feeling comfortable talking with patients about ED behaviors (n = 28, 30%).
Fig. 2
a Physicians’ self-reported practices regarding diagnosis and treatment of EDs in general and in RESGM populations (n = 92). b Self-reported practices related to ED diagnosis and management among physicians who received ED training at their current residency program (n = 21). c Self-reported preferences for further sensitivity training regarding the treatment of EDs in diverse populations (n = 92)
Perceived barriers to access to mental healthcareFigure 3a demonstrates that the top two barriers for sexual and gender minoritized patients seeking ED treatment perceived by resident trainees were “mistrust of the healthcare system,” selected (n = 32, 35%), followed by “stigma”, selected (n = 28, 30%) times. With regard to racial and ethnic minoritized patients, Fig. 3b illustrates that the top two barriers for racial and ethnic minoritized patients seeking ED treatment perceived by resident trainees were “stigma”, selected (n = 31, 34%) and “mistrust of the healthcare system”, selected (n = 29, 32%) times. The third highest barrier selected by trainees was “none”, selected (n = 27, 30%) times.
Fig. 3
Resident-reported perceived barriers faced by a racial and ethnic minoritized, b sexual and gender minoritized individuals receiving care for EDs
留言 (0)