This study examined whether child and parental psychosocial factors were cross-sectionally associated with BE and whether BE was associated with BMIz and waist circumference cross-sectionally and longitudinally among young Finnish adolescents. The prevalence of BE was 1.8% at baseline. Low self-esteem and other disordered eating attitudes and behaviors were associated with greater odds for child BE when adjusting for the child’s BMIz. Child and parental body dissatisfaction were associated with higher odds of BE, but not after adjusting for child BMIz. As expected, BE was associated with higher BMIz and waist circumference cross-sectionally and longitudinally after a 2.6-year follow-up, although the association was diluted at follow-up.
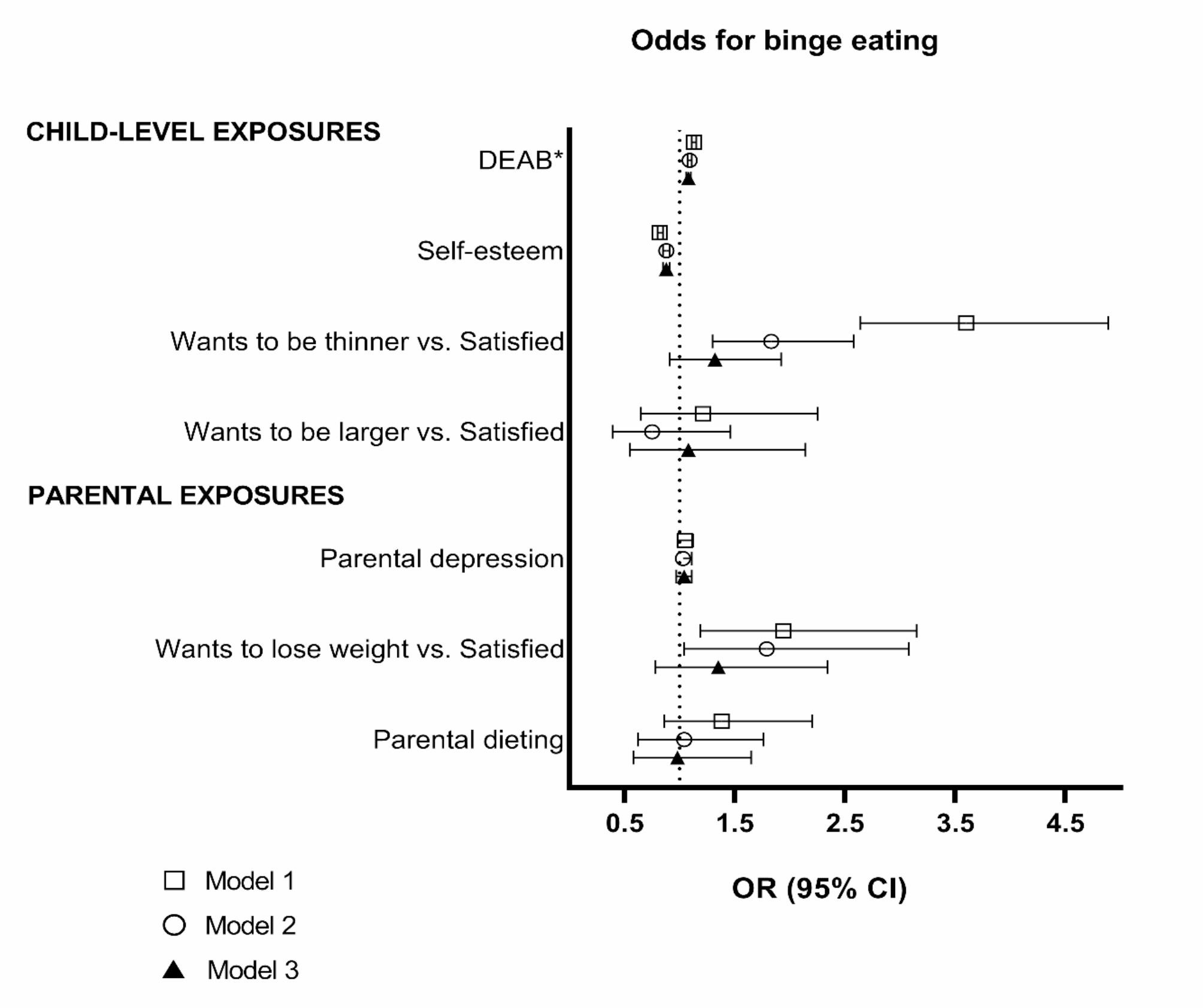
Similarly to our results, low self-esteem has been found to be associated with and to predict binge and LOC eating in several studies among children and adolescents [2, 9, 14]. In previous studies, low self-esteem has also been associated with body dissatisfaction and, e.g., depression, and these factors together may mediate the effects of one another on BE. For example, self-esteem and depression have been found to mediate associations between body dissatisfaction and BE [14, 39, 40]. Additionally, according to research findings, physical appearance is a component of general self-esteem [41]. Thus, it is noteworthy that in our analyses, contrary to Brechan et al. (2015), the associations between self-esteem and body dissatisfaction also remained significant when analyzed together, showing independent associations between them and BE. As expected, other DEABs were also associated with higher odds of BE. Previous studies have also revealed that different disordered eating symptoms often coexist and may contribute to each other, e.g., dietary restraint and BE [8,9,10, 12].
We found that wanting to be thinner was associated with higher odds of BE, but the association was attenuated after controlling for BMIz. Wanting to be larger was not associated with BE. Many previous studies, both cross-sectional and longitudinal, have reported similar associations, but mostly no adjustments with weight status have been made [2, 9, 12, 14, 39, 42]. Studies exploring body image have mostly used statements that have referred to wanting to be thinner, or no distinction between wanting to be thinner or larger has been made [2, 9, 12, 14]. The disappearance of the association after adjustment for BMIz suggests that BMIz explained the association between body dissatisfaction and BE. Body dissatisfaction as a determinant of BE may be especially pronounced among adolescents with higher weight, but other determinants may be more important for normal weight adolescents with BE. Thus, stratified analyses based on weight status may be warranted.
In summary, the current results suggest that low self-esteem, body dissatisfaction, and overall disordered eating attitudes and behaviors play important roles in adolescent BE. Binge eating is a multifaceted behavior influenced by various factors, including psychological, social, biological, and environmental aspects. Therefore, holistic approach is needed when assessing risks or developing preventive interventions for binge eating. Low self-esteem, overall disordered eating attitudes, and body dissatisfaction may be important driving forces, but they cannot be seen as the only ones. With respect to prevention, body image and self-esteem have been targeted in interventions aiming to prevent eating disorders among children and adolescents with some success [43,44,45].
The associations between binge and LOC eating and higher BMI have been reported in many studies [2, 10, 12, 18], including ours. In addition, among youth with obesity, LOC eating is a common feature, as one quarter of children and adolescents with overweight and obesity demonstrate LOC eating [46]. This association may also be bidirectional, as overweight can be a consequence of BE as well as a factor contributing to it [2, 12, 18], e.g., due to dieting attempts [47] or weight bullying/negative comments predisposing individuals to BE [48]. The genetic predisposition to overweight may also play a role, as it has been found to be associated with BE [49]. In this study, BE was strongly associated with higher BMI and waist circumference cross-sectionally, and it also predicted higher BMI and waist circumference, although the impact was diluted, predicting only 0.14 units higher BMIz and 1.1 cm larger waist circumference after follow-up. This may be due to possible changes in BE or other disordered eating behaviors during the follow-up, which we were unfortunately unable to consider due to a lack of data.
We found little evidence that potential parental correlates are associated with child BE, as neither parental depressive symptoms nor dieting were associated with child BE in the current study. Similarly, maternal or paternal depressive symptoms were not associated with child LOC or BE in a Dutch study of 14-year-olds, although the authors state that these results should be interpreted with caution because of the use of a possibly selective sample [12]. Martinson et al. (2016) reported that parental depression and anxiety were associated with adolescent DEAB, but only among adolescents with poorer emotional awareness/expression [25]. The prevalence of having any eating disorder was elevated among 12–24-year-old offspring of parents with a diagnosed mental illness [24]. Thus, the role of parental depression in child BE needs further clarification.
In this study, parental weight dissatisfaction was associated with higher odds for child BE, but the association was attenuated after controlling for child BMIz. Parental and child BMIs as well as parental and child body dissatisfaction are probably intertwined and may together predispose the child to BE. In this study, children of parents with weight dissatisfaction had higher BMIz values and wanted to be thinner more likely than children of parents who were satisfied with their weight (data not shown). Previous results have shown that such indirect encouragement to lose weight, such as maternal/parental body dissatisfaction, weight concerns, and dieting, is deleterious for a child’s body image and eating behaviors and attitudes, especially among daughters [22, 50,51,52]. Our results partly support these findings but also stress the importance of the child’s and perhaps also the parent’s weight status in this matter.
The prevalence of BE in the present study, 1.8%, was lower than that reported in other studies on adolescents. In other community sample studies, the prevalence has varied between 2.2% and over 20% among US, German, Dutch, and Italian adolescents [2, 12,13,14,15]. The low prevalence might be due to the young study population, as the prevalence of BE usually peaks in late adolescence [13], or somewhat different assessment methods. We found no other Finnish or Nordic studies for comparison.
The findings of the study, together with previous studies, highlight the need for preventive measures in families, schools and among health care practitioners to support good self-esteem, positive body image, and healthy eating behaviors and attitudes among adolescents. In addition, scalable preventive interventions targeting these determinants are also needed.
Strengths and limitations
A strength of the study is the large and geographically diverse sample, although the sample is not representative of all Finnish 9–12-year-olds owing to the higher socioeconomic background of the families compared with the general population [53]. Another strength is the use of validated questions and questionnaires concerning BE, DEAB, and self-esteem [27, 32, 54]. The study also adds to the previous literature, as there are very few studies on child/adolescent BE and its determinants in Finland and other Nordic countries.
Although validated, the use of the two-item assessment method to assess BE can also be seen as a limitation. Using structured interviews would be the best option to assess BE among youth, as they may have difficulty identifying BE episodes when they do not receive detailed instructions [55]. This limitation concerns most questionnaire-based studies, as BE is usually estimated with two questions: one on the amount of food eaten and the other on the feeling of loss of control. Another limitation is the descriptive nature of most of the analyses. There is a possibility for inverse causality concerning the child’s psychosocial determinants of BE and its cross-sectional associations with obesity indicators, although the results of other studies shed light on the direction of the associations.




留言 (0)