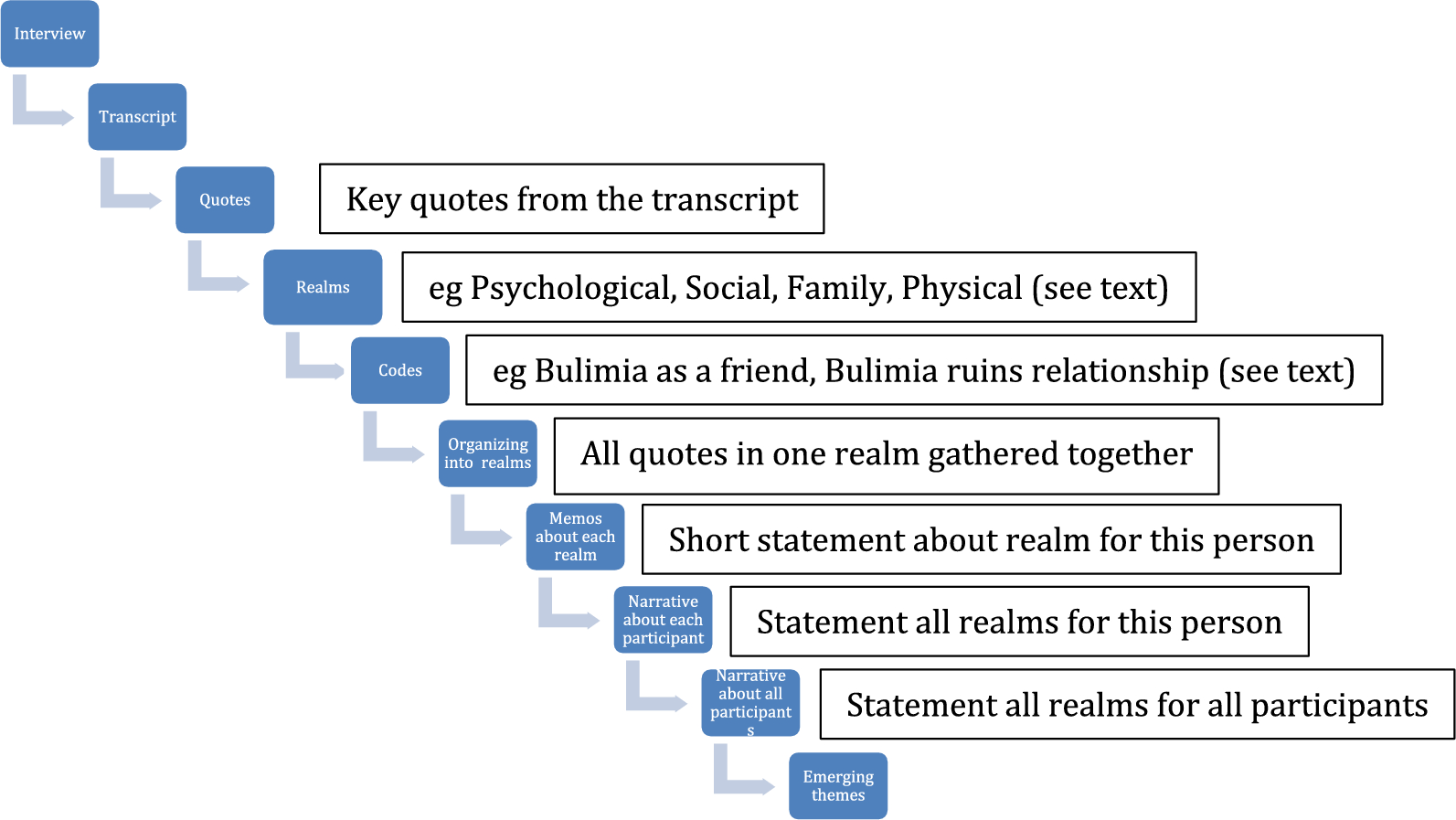
Reflexive thematic analysis [2, 3] of the data produced four connected themes contributing to understanding autonomy of people with lived experience of longstanding EDs and what this means for their treatment and recovery. The four themes, Self versus ED; Self in Treatment; Self in Recovery; and Self in Relation to Others are represented in Table 4, alongside thirteen subthemes. Following a description of each theme, the relational connections across these four themes are presented as a conceptual finding; the Lack of Autonomy Loop. Reflexive analysis of the four themes show being stuck in a lack of autonomy loop acts as a barrier to treatment and recovery while paradoxically asking for help, and freely surrendering control may facilitate increased autonomy and self-agency, facilitating treatment and recovery. Importantly, the findings identify features of autonomy and relationships that support treatment and recovery through fostering increased safety, trust, and collaboration.
Table 4 Breakdown of review results by themeAccess to qualitative, quantitative, and mixed-methods data sets was a strength of the study. The first author developed theme names to succinctly summarise the themes, while lived experience participant quotes extracted from the selected studies, were provided to exemplify and describe each theme. As themes three and four were derived mainly from a thematic synthesis of the research findings of the selected studies, these themes used less extracted lived experience quotes. Each theme begins with a description of the theme and discussion of the findings of qualitative and lived experience data and concludes with a summary of the statistical support provided by the quantitative studies included in that theme.
Self versus eating disorder
Self versus ED appeared across 17 of the included articles [1, 80,81,82, 84, 85, 87, 88, 90,91,92,93,94,95,96,97,98] (ten qualitative, five quantitative, and two mixed-methods) and personifies a struggle between the Self and the ED. This theme portrays the internal conflict between two opposing forces: the individual's yearning for a fulfilling life and the EDs relentless pursuit of control.
ED in charge appeared across nine studies [1, 80,81,82, 84, 85, 87, 90, 93] and refers to feeling disconnected from the self and life; imprisoned by the ED. It includes findings where the ED contributes to experiences of suicide, isolation, and distress.
…disgust with myself, endless suffering…it is awful when you cannot stand yourself, who you are, the struggles, the continual losing battles to binges (Inès) [84 p. 3].
I was waiting for the right moment when I could commit suicide...I knew for sure that I could not go on living if things were to continue to be like this (Linnéa) [85 p. 864].
…this wretched thing has taken over my life, destroying me, cutting me off from the world, from my family and from life (Léa) [84 p. 4].
Feeling stuck in the ED appeared across ten studies [80, 81, 83, 84, 86, 89, 91, 92, 94, 97], describing participants’ ambivalence towards change and coinciding fluctuations in motivation for recovery, their relationship with the illness, and lengthy treatments where no progress is made. Other people may assume control and arrange hospitalisation when they see the person suffering; however, this leads to increased powerlessness, isolation, and a further lack of connection.
…I had dozens of hospital admissions with no success…Treatment felt like banging my head against a brick wall (Olivia) [81 p. 499].
…I want to be able to be happy, only I’m afraid for myself because I’m so ambivalent. I have the constant feeling that two beings are constantly struggling inside me: Marie and the anorexic (Marie) [84 p. 4].
Self is called to action appeared across six studies [80, 81, 83, 84, 86, 94] and refers to internal or external processes that trigger change, with a different and more autonomous quality of motivation.
That day a man died from [ED] in the hospital. It became very clear to me then that you could die from [ED]...It hit me that I wasn’t normal, and I was so sick of battling my brain. I had to [decide]: Am I going to let myself die, or am I going to beat this and make a go of my life? I made a conscious decision to get better. That day was a turning point (Ruby) [81 p. 501].
As Dawson and colleagues [80] explain the illness can change from being perceived as something of potential value to something destructive and futile due to the ED’s severity and a growing awareness of the long-term impact. Life with ED can become untenable, with change the only option:
It was something I had to make a choice to do, and I made that choice because I didn’t want to be a prisoner anymore (Emily) [81 p. 501].
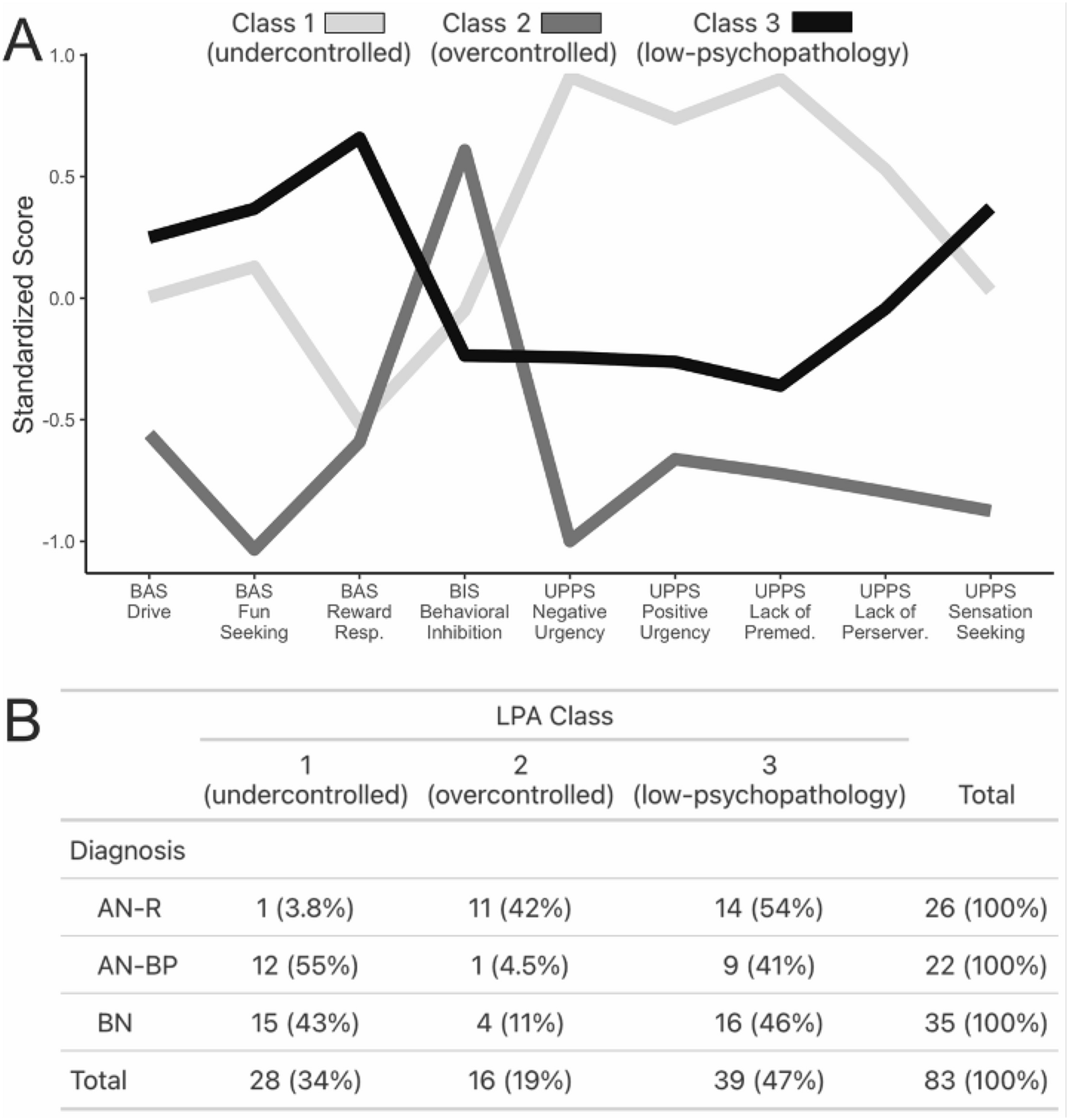
Findings from five quantitative [91, 94,95,96, 98] and two mixed-methods [80, 97] studies are consistent with these qualitative findings, highlighting persistent barriers to change even when individuals are ready to embark on recovery. Tomba and colleagues [96] found significant differences in psychological well-being between 245 outpatients and 60 community controls, underscoring the distress permeating across the lives of those with EDs. Strand and colleagues [1] reported that while self-admission contracts reduced hospitalisation by 50% at 12-month follow-up, they were not associated with improvements in ED morbidity or BMI.
Self in treatment
Self in Treatment emerged as a major theme across 19 articles [1, 80,81,82,83, 85,86,87,88,89,90,91,92,93,94,95,96,97,98] (nine qualitative, eight quantitative, two mixed-methods) and refers to the experiences and impacts of treatment delivery and how people living with an ED experience the process of treatment.
Coercion and control appeared across six studies [80, 81, 88, 93, 97, 98]. This encompasses a lack of collaboration and involvement in treatment decisions, the importance of relationships with the treatment team and promoting client agency. In their mixed-methods study, Darcy and colleagues [80] report that the majority of participants were not involved in any treatment-related decisions.
I feel I am out of the loop and I find that it makes me feel really anxious…everyone is deciding what is happening and nobody is asking me (Elsie) [93 p. 21].
Although coercive practices and therapeutic alliances were not the focus of this study, their pervasive presence in the autonomy literature signals the systemic and widespread nature of such practices in ED treatment. The analysis revealed a spectrum of experiences, from feelings of exclusion and powerlessness to encounters with coercive and punitive treatment processes. These experiences often left individuals clinging to their EDs as a last resort for maintaining a sense of control in an environment where their autonomy was repeatedly undermined:
But the punitive thing…that just fuels the disease, that does nothing helpful (Madison) [80 p. 267].
If the clinicians told me what to do I’d think, ‘Well screw you. I’m not doing that.’...It became more about the ‘us’ and ‘them’ (Amelia) [81 p. 499].
Autonomy Support appeared across 16 articles [1, 80,81,82, 85,86,87,88,89,90,91, 93,94,95, 97, 98] and refers to delivering treatment in a manner that is informative and free of threats, coercion and/or force to achieve compliance [91]. Being heard, feeling like your experience matters and someone is listening, promotes a sense of collaboration and autonomy:
The key factor in motivating me to change my outlook and increase my propensity to challenge anxious and depressive traits has been the relinquished agenda of forced treatment in exchange for a non-threatening and comprehensive, interactive treatment plan..... that seeks nothing more than to provide support, one that meets me where I’m at (Julie) [98 p. 94].
Freely choosing to engage in treatment, being supported to do so, and having individualised treatment options available and accessible like self-admission, can significantly enhance a person’s sense of autonomy:
Even if I don’t do everything with joy when I’m [at the ward], I know that I’m doing it because I’ve chosen it myself. And then maybe I can show others that have even greater difficulties that it’s possible to do it by your own free will…[sic] (Kalle) [1 p. 404].
…it affects my everyday life 24/7, just knowing that I have the opportunity [to self-admit if needed] (Misha) [1 p. 402].
Partnering to reduce harm refers to people with EDs collaborating with care providers to reduce the negative impact of the disorder and improve their quality of life [51]. One example from this review is the Community Outreach Partnership Program (COPP) discussed by Williams and colleagues [98]. In this approach, the individual is at the centre of all decision-making and the team works alongside them to achieve their personally identified goals, which may or may not align with traditional treatment objectives [98]. A second example is Strand and colleagues’ [1] study of freedom to self-admit which demonstrably reduces the length of time as an inpatient and prevents deterioration. This harm-reductive approach affords access to treatment before deterioration, and participants reported that simply knowing this option was available provided an “enormous sense of security” [1 p. 402]. Two further studies [83, 89] showed the benefits of non-coercive treatment approaches and demonstrated movement towards autonomy-supportive treatment.
Awareness of Self and Disorder appeared across five studies [84, 88, 92, 93, 98] and refers to increased insight into the disorder's underlying cause and function. For many, EDs develop as a response to traumatic experiences:
I started to become aware that the [ED] wasn’t a choice— it was a reaction. As a teenage girl, the only thing I could control was my body because I had no power. Exploring the issues behind the [ED] was helpful for me—knowing where my need to be perfect came from and realizing that I achieved perfection through eating (Jessica) [




留言 (0)