Biospecimen collection
The study was conducted in adherence to the Declaration of Helsinki and approved by the medical ethics committee at the West China Hospital, Sichuan University. Plasma samples were collected from healthy controls (HC = 30) and patients with pancreatic cancer (PDAC = 100) and stored at -80 ℃ before use. Written informed consent was obtained from all participants.
This prospective observational study collected plasma samples from patients admitted to the Department of Pancreatic Surgery of West China Hospital between June 2020 and May 2022. The inclusion criteria were as follows: (1) be over 18 years of age, (2) have accurate Chinese character writing ability, (3) be proficient in oral expression, (4) have no history of mental illness, (5) understand the purpose and content of the study, (6) be able to sign informed consent, and (7) have been diagnosed with PDAC for the first time in the Department of Pancreatic Surgery at West China Hospital of Sichuan University. The diagnostic gold standard was based on pathological diagnosis of intraoperative tissue samples. The exclusion criteria were as follows: (1) those with non-primary pancreatic tumors or with two or more types of tumors including pancreatic cancer, (2) those with a history of tumor or chemoradiotherapy, (3) those who need to take immunosuppressants or hormones for an extended period due to disease, and (4) those diagnosed with kidney disease such as nephrotic syndrome, IgA nephropathy, acute or chronic renal insufficiency, etc. (5) other pancreatic borderline or benign tumors include intraductal papillary mucinous neoplasm, pancreatic serous or mucinous cystadenoma, solid pseudopapillary tumor of the pancreas, and pancreatic neuroendocrine tumor.
Plasma samples were collected from patients diagnosed with PDAC prior to surgery. Mass spectrometry was performed after postoperative pathological diagnosis confirmed PDAC, with the consent of patients and their families.
Clinical data collection
The clinical data collected from patients included their age, sex, body mass index (BMI), hypertension, diabetes, smoking and drinking habits, jaundice, CA19-9 levels, tumor size, tumor location (head of pancreas, uncinate process of pancreas, neck of pancreas, body of pancreas, and tail of pancreas), and stage of PDAC. The classification and staging of PDAC were performed according to the (tumor–node–metastasis) TNM staging and the American joint committee on cancer (AJCC) staging (stage I, II, III, IV), edition 8 [26].
Preparation of IgG
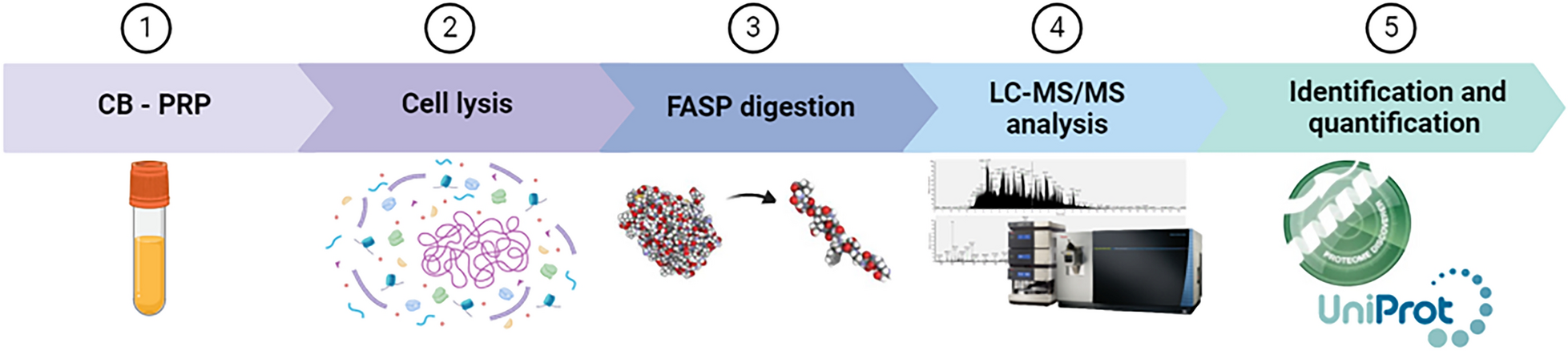
Plasma IgG from 130 samples were purified using our optimized method previously described. In brief, we mixed 20 µL of plasma in a microcentrifuge tube with 40 µL of equilibrated immobilized protein A/G agarose. The mixture was then incubated with 200 µL of binding buffer (25 mM tristate buffer, 150 mM sodium chloride, pH7.2) for 2 h at 4 ℃ on a rotator. After a brief centrifugation, the supernatant was discarded, and we added approximately 500 µL of binding buffer to wash the unbound proteins. Subsequently, 50 µL of elution buffer (0.1 M formic acid) was added to release the captured plasma IgGs. The tube was incubated for 5 min at 25 ℃ on a rotator, and then briefly centrifuged to collect purified IgGs. Quantification was performed using the bicinchoninic acid protein assay at 562 nm.
Denature, reduction, alkylation and digestion
The 20 µg of IgGs was added to 200 µL of 50 mM ammonium bicarbonate (ABC) buffer (pH8.5), and the mixture was denatured by heating at 95 ℃ for 10 min. The protein was then reduced and alkylated by adding 4 µL of 1 M dithiothreitol for 45 min at 56 ℃, followed by 10 µL of 1 M iodoacetamide (IAM) for 30 min at 25 ℃ in the dark. The resulting mixture was then loaded into a 10 kDa ultrafiltration tube (Millipore Corporation, Billerica). The agents were subsequently replaced with ABC buffer three times and centrifuged at 13,000 g for 10 min. Next, approximately 500 ng of trypsin and 100 µL of ABC were added and oscillated overnight at 37 ℃. The digests were collected by centrifugation at 13,000 g for 10 min at 4 ℃. Finally, the peptides were dried using the SpeedVac and stored at -80 ℃ for further analysis.
LC-MS/MS analysis
The peptides from each sample were resuspended in 40 µL of 0.1% formic acid. Subsequently, 1 µL of peptides was separated on a ReproSil-Pur C18-AQ column (1.9 μm, 100 μm inner diameter, length 25 cm; Dr Maisch) using a 30-min gradient (0–2 min, 5–12% B; 2–7 min, 12–22% B; 7–21 min, 22–32% B; 21–22 min, 32–90% B; 22–30 min, 90% B) at a flow rate of 350 nL/min. Finally, the separated peptides were analyzed using an Orbitrap Fusion Lumos Mass Spectrometer (Thermo Fisher, USA).
An alternative fragmentation between the EThcD and sceHCD modes was used in a duty cycle of 3 s for EThcD-sceHCD-MS/MS. During the EThcD duty cycle of 2 s, MS1 was analyzed at an Orbitrap resolution of 60,000 within the 400–1600 m/z range. The RF lens, AGC target, MIT, and exclusion duration were set to 40%, 2.0 e5, 50 ms, and 15 s, respectively. MS2 was analyzed at an Orbitrap resolution of 30,000 with 2 m/z. The AGC target, MIT, and EThcD type were standard, 150 ms, and 35%, respectively. During the sceHCD duty cycle of 1 s, MS1 was analyzed using a range of 400–1600 m/z at an Orbitrap resolution of 60,000. The RF lens, AGC target, MIT, and exclusion duration were set to 40%, standard, auto, and 15 s, respectively. MS2 was analyzed with a resolution of 30,000 at 1.6 m/z. The AGC target, MIT, and HCD collision energies were set to standard, auto, and 30%, respectively. Additionally, the sceHCD mode was enabled with an energy difference of ± 10% (20-30-40%).
Data analysis and bioinformatics
Byonic software (version 3.10.10, Protein Metrics, Inc.) was used to search the RAW data files. The human IgG Uniprot database was selected. Precursor and fragment ion mass tolerances were set as ± 6 ppm and ± 20 ppm, respectively. The fragmentation type was set to “Both HCD & EThcD”. Two missed cleavage sites were allowed. Carbamidomethyl (C) was set as a fixed modification, while Oxidation (M) and Acetyl (Protein N-term) were set as variable modifications. The N-glycan modification was set as the “182 human N-glycans”. Protein groups were filtered to 1% FDR. Quality control methods for identifying intact N-glycopeptides included a Byonic score of over 200 and at least 5 amino acids. Each spectrum of intact N-glycopeptide should be confirmed manually. Abnormal data were initially excluded based on the spectral shape and TIC information. The remaining data was classified into five groups (HC, PDAC I, PDAC II, PDAC III, and PDAC IV) according to clinical information.
The intact N-glycopeptides were quantified using PANDA software (v.1.2.5) in label-free quantification mode with or without the match between runs (MBR) function. Both MS raw files and “output.spectra” files (intact glycopeptide identification files obtained from the Byonic search results) were imported. Default values were used for all other parameters. The batch search results were compiled into a file named “Peptides_F1” using PANDA. The file can be used for qualitative comparison without MBR. To compare the detection rate of N-glycopeptide between HC and PDAC patients, those glycopeptides whose detection rate ≤ 50% in both of the two groups were removed, and Chi-square was employed to calculate the p-value. For remaining glycopeptides, MBR was selected to supplement missing quantitative values. In addition, the remaining missing values were filled with the minimum value. Furtherly, the data of each column was normalized (the ratio of glycopeptide expression to total expression per column can be calculated as the glycopeptide ratio). Finally, glycopeptides were accumulated by site-specificity for further analysis.
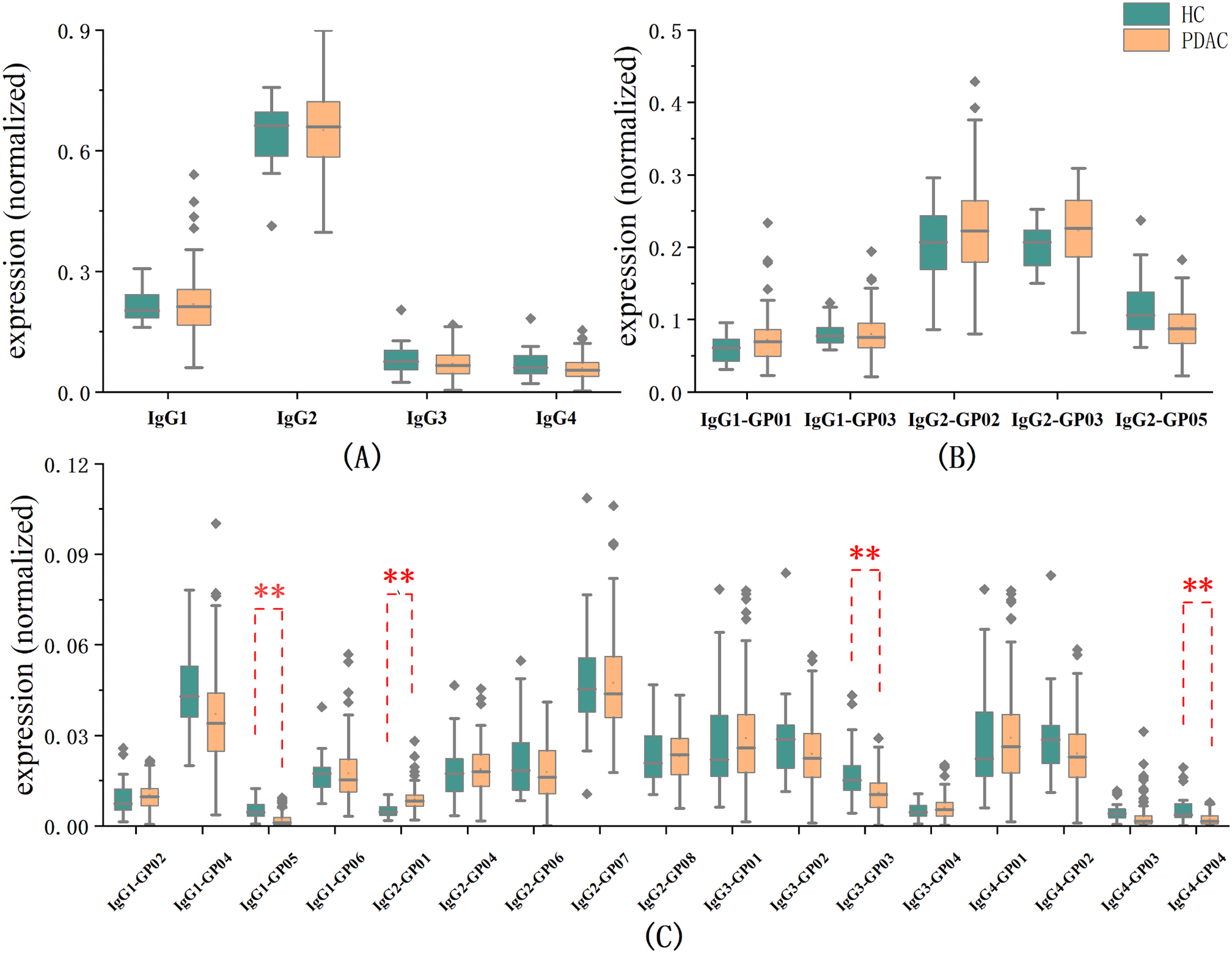
There were two groups, HC and PDAC. The study compared the expression level of four glycopeptides subclasses and intact N- glycopeptides obtained by site-specific accumulation in the two groups using grouped boxplots. Hypothesis testing was then used to compare the expression of glycopeptides between the two groups in the Wukong platform. Statistical significance was defined as p < 0.05. FC (fold change) >1.5 indicates up-regulated expression, while FC<0.67 indicates down-regulated expression. The boxplots with statistical significance were marked. The correlation between differential glycopeptides and clinical information including serum CA19-9 level, BMI, and age was analyzed using the Spearman correlation method in Origin (2021). The patients were divided into two groups based on gender and jaundice. The t-test (p < 0.05) and fold change (FC > 1.5 or < 0.67) were used to determine whether there was a difference in the expression of differential glycopeptides between two groups. Binary logistic regression was used to perform univariate and multivariate analyses in SPSS (v.27) to establish a diagnostic model for PDAC patients compared to HC. Besides, K-fold cross validation was used to evaluate the model (k = 10). Subsequently, the multivariate diagnosis of pancreatic cancer was performed using receiver operating characteristic (ROC) analysis. Patients were followed up until January 31st, 2024. The Cox proportional hazards model was employed to analyze factors associated with prognosis. Statistical significance was defined as p < 0.05.



留言 (0)