The accurate and rapid diagnosis of TB, especially at the point-of-care, is crucial for curbing the spread of the disease, treatment monitoring, risk analysis and prognosis [9]. A pressing challenge in TB diagnosis lies in the development of more streamlined, accurate, and rapid point-of-care tests [17]. Although efforts to develop novel tools for infectious disease diagnosis have been focused on discovery of single disease-specific biomarkers, this focus will likely shift towards discovery of bio-profiles or biosignatures comprised of well-defined sets of reliable molecular indicators [18]. In the present study, we identified five urine proteins with strong potential applicability as single PTB-diagnostic biomarkers (CPB2, HTRA1, HEXA, FLNA, NRP1) that all yielded AUCs of > 0.80. Notably, a five-marker biosignature incorporating the same proteins effectively distinguished PTB from CAP, LCA, and HC, as based on AUCs of 0.9680, 0.9310, and 0.9840, respectively. However, the use of individual proteins as diagnostic tools for infectious diseases such as PTB is not generally recommended, since single inflammatory biomarkers tend to have low disease specificities [19]. As expected, our study demonstrated superior PTB-diagnostic accuracies of biomarker combinations as compared to individual markers, as reflected by EFS ranking and Student’s t-test results, as observed in previous studies [20,21,22].
Meanwhile, our results also indicate that proteomics is valuable tool for achieving effective PTB diagnosis and differential diagnosis, as consistent with results obtained by Liu et al. who analyzed and compared urinary proteomic profiles of TB patients and healthy controls. They found that the combined set of P22352, Q9P121, P15151, Q13291, and Q8NDA2 biomarkers could be useful for diagnosing TB, as based on a TB-diagnostic sensitivity rate of 82.70% and latent TB infection (LTBI)-diagnostic specificity rate of 92.30% [20]. Recently, P01011, Q8NCW5, P28072, A0A2Q2TTZ9, and Q99574 were identified via MS conducted using a Q-Exactive Orbitrap mass spectrometer then these biomarkers were combined to generate a five-protein biosignature that, after leave-one-out cross-validation, yielded an AUC of 1.00 (95% CI, 1.00–1.00) and exhibited a TB-diagnostic sensitivity rate of 100% (95% CI, 76.20–100%) and specificity rate of 90.9% (95% CI, 58.70–99.80%) [21]. One important issue is that biomarkers from different studies rarely overlap even when the groups to be compared are the same. The reasons can be the small sample size, statistical fluctuations in individual systemic biological state, race factor, experimental conditions, and analytical apparatuses differ from one study to another [9, 22]. However, one must consider the possibility that multiple independent systemic regulated states exist, each manifesting the same typical TB symptoms, yet none of the biomarkers are consistently up- or down-regulated across these different states. This is akin to a non-linear complex equation often having multiple solutions [9].
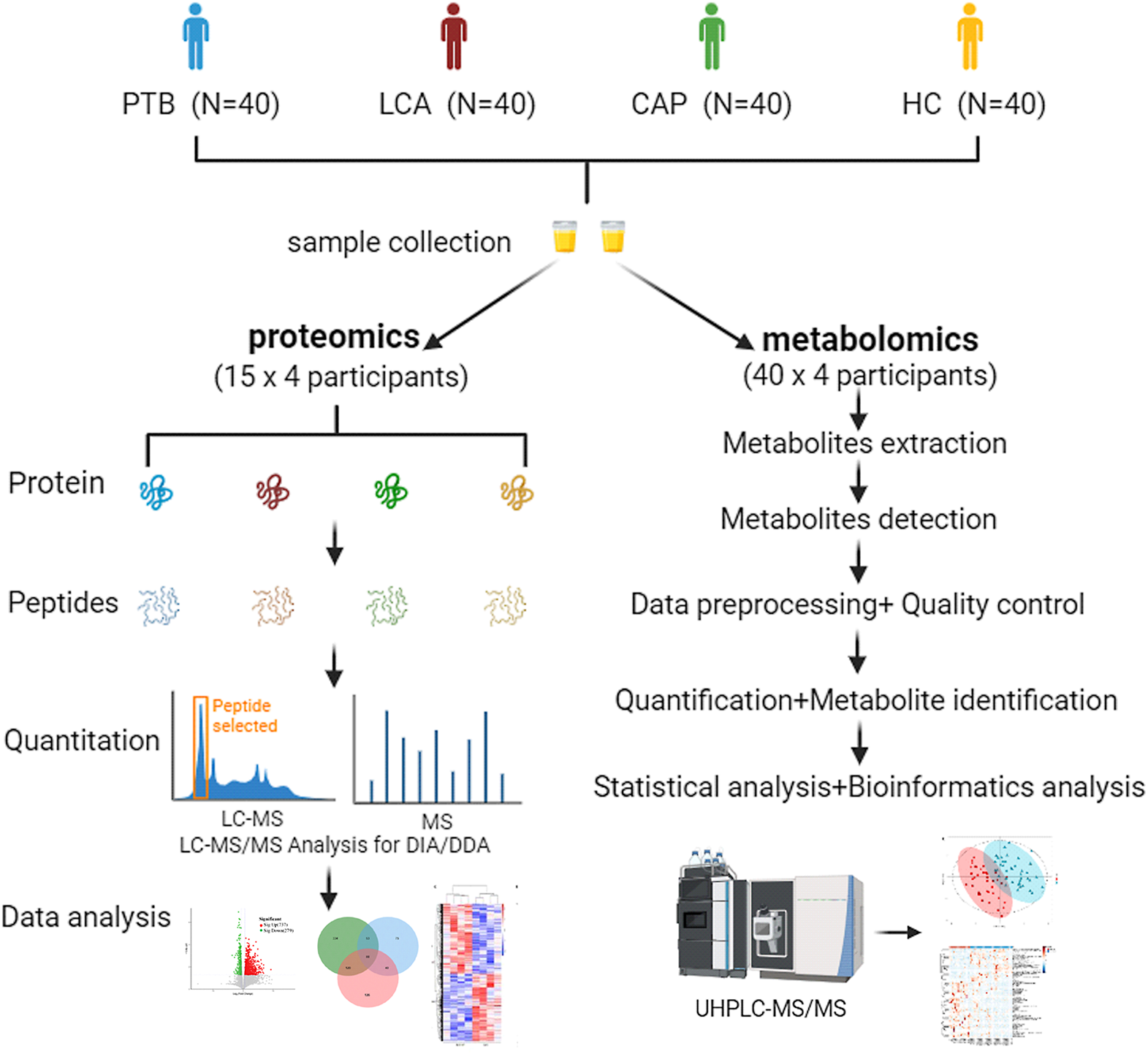
Metabolomics, like proteomics, has been increasingly used for PTB diagnosis in recent years. For example, in 2014–2015, Mrinal et al. [23] and Mahapatra et al. [24] reported that LC-MS and gas chromatography-mass spectrometry methods, respectively, could be used to identify metabolites in urine samples of TB patients. Since then, a multitude of metabolomics-based studies have been reported describing the successful use of small molecule metabolites as urine PTB-diagnostic biomarkers [10]. However, these studies only explored a subset of all potential PTB-predictive DAMs in urine of PTB patients, as LC-MS detection of all urinary compounds is not yet feasible. To broaden our repertoire of identified metabolites, we employed ultra-high-performance liquid chromatography (UHPLC)-MS/MS techniques to screen for DAMs present in urine specimens of PTB, LCA, CAP, and HC groups. Our findings pinpointed five potentially useful PTB-diagnostic and differentially diagnostic DAMs for each group, as based on AUCs of ≥ 0.71 and p values of < 0.01. Interestingly, a biosignature incorporating the five metabolite biomarkers was capable of effectively differentiating PTB from CAP, LCA, and HC, as based on respective AUCs of 0.8920, 0.8570, and 0.9940. These DAMs are mainly by-products of amino acid, nucleotide, and lipid metabolism and are often generated during oxidative stress and inflammatory responses [10, 25,26,27].
In a similar vein, metabolomics results obtained by Jiang et al. [25] and Cho et al. [27] demonstrated that changes in blood serum levels of multiple amino acids in active TB patients may serve as useful biomarkers for achieving adjunctive, rapid, and noninvasive PTB diagnosis. Oleamide has been shown to be a useful biomarker for distinguishing between tuberculous pleural effusion and malignant pleural effusion [28]. Furthermore, a biosignature incorporating these three metabolites effectively discriminated between TB patients and HCs (AUC = 0.97). Another noteworthy study highlighted the potential of free 3-NT levels in biological samples to differentiate drug-sensitive TB from drug-resistant TB [26]. More recently, a nuclear magnetic resonance-based urinary metabolomics study identified eight metabolites; a urine metabolic fingerprint based on these metabolites could be used to effectively discriminate active TB patients from pneumococcal pneumonia patients, those with LTBI, and HCs [10]. This urinary metabolic fingerprint may also be capable of distinguishing PTB patients from HCs, LCA patients, and CAP patients and thus may be a useful noninvasive biosignature for achieving effective PTB diagnosis and differential diagnosis, warranting further research.
Importantly, different omics methodologies detect different subsets of diagnostic biomarkers present in complex clinical specimens. In fact, the power of Multi-omics approach has already been shown by in vivo and in vitro modelling studies that reconciled multilayered omics data acquisitions and metabolic and other phenotypes over a large number of experiments (performed in different conditions) and were able to accurately predict biological behavior [29]. Here, we integrated proteomics and metabolomics to discover urine PTB-diagnostic biomarkers (five proteins and five metabolites) using pairwise comparisons of biomarkers of PTB, LCA, CAP, and HC groups. As an additional contribution, we present a multi-omics-derived PTB-diagnostic biomarker signature, a rarity in the literature. In addition, the quantification of statistically significant biomarkers identified in Multi-omics would allow this technology to be adapted to a point-of-care test, especially in resource-constrained settings. This study had several limitations. First, the number of urine specimens subjected to proteomics and metabolomics analyses was relatively small and thus prevented us from ruling out potential bias due to sample heterogeneity, an issue that can be addressed through validation of biomarkers using large sample sets. Second, although we included samples based on our criteria for our comparative analyses, additional undetected, uncontrolled genetic, clinical, or environmental confounding factors may have influenced our results. Third, the clinical efficacy of biomarkers identified in our cohort was also not assessed in a larger population; thus, further validation is urgently required. Finally, due to the lack of our ability to interpret the complex nature and biological mechanisms of metabolism between diverse analytes, we focused on the analysis of diagnostic performance to the five protein and five metabolism biomarkers, we made the raw data publicly available.






留言 (0)