Participants
In this cross-sectional study, 38 participants were enrolled from an ongoing prospective dementia cohort at Peking Union Medical University Hospital (PUMCH). The PUMCH Dementia Cohort is a hospital-based, observational study of subjects with cognitive impairment and cognitive normal healthy volunteers. The aims and eligibility criteria of the original study are described on ClinicalTrials. gov (NCT05023564). All participants underwent detailed clinical examination, neuropsychological battery tests, blood biochemical tests, CSF testing, APOE genotyping, and neuroimaging assessments [24].
The study included 29 patients in the Alzheimer’s continuum according to the National Institute on Aging and Alzheimer’s Association (NIA-AA) 2018 framework with clinical diagnosis of AD or mild cognitive impairment (MCI) due to AD [3]; 5 patients with frontotemporal dementia according to Diagnostic and Statistical Manual of Mental Disorders, 5th Edition [25]; 1 patient with progressive supranuclear palsy based on the 2017 Hoglinger criteria [26]; 1 patient with Creutzfeldt-jakob disease; 1 patient with dementia of undetermined cause; and 1 healthy volunteer. All participants underwent [18F]florbetapir PET scan on the uMI Panorama PET/CT scanner between January 2023 and December 2023, along with a T1-weighted brain MRI scan within three days. The study received approval from the ethics committee of the PUMCH and was conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all subjects or caregivers.
Image acquisition
Each participant underwent a routine brain PET scan 50 min after receiving an intravenous injection of [18F]florbetapir (median [inter-quantile range]: 308.95 [284.90, 341.33 MBq]), using the digital uMI Panorama PET/CT scanner (United Imaging Healthcare). Prior to PET acquisition, a low-dose CT scan was performed for attenuation correction. Corrections for randoms, attenuation, scatter, normalization, decay, and dead time were applied during the reconstruction. The list-mode PET data were reconstructed into varying durations: 10 min, 2 min, 1 min, 45 s, and 30 s (G10min, G2min, G1min, G45s, G30s). All PET images were reconstructed using a 3D-ordered subset expectation maximization algorithm with point spread function and TOF modeling. The reconstruction parameters were set at 4 iterations, 10 subsets, a 192 × 192 matrix, a 300 mm field of view (FOV), a 1.56 mm slice thickness, and a Gaussian post-filter with 5 mm of full-width half maximum. Additionally, high-resolution brain MR T1 images with a resolution of 1 × 1 × 1 mm³ were acquired using a fast spoiled gradient-echo sequence on a 3T MRI scanner (uPMR790, United Imaging Healthcare) for all subjects.
Subjective visual assessment
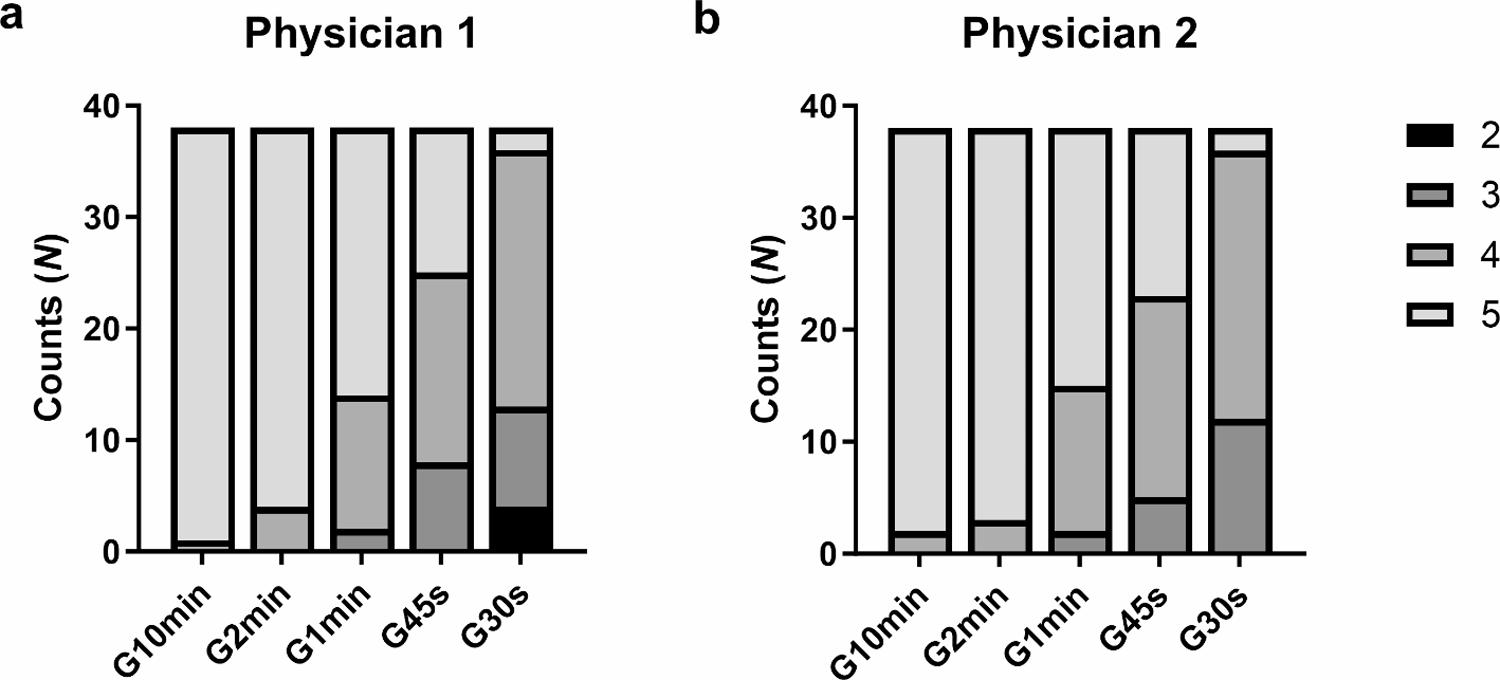
Two trained nuclear medicine physicians, blinded to all clinical and diagnostic information, independently visually assessed all PET images presented in randomized order. Each [18F]florbetapir PET image was given a binary diagnosis of Aβ status (Aβ positive or Aβ negative) based on the manufacturer’s reading guideline [27]. The G10min group’s diagnostic results served as the ground truth for each participant. In cases of disagreements in the visual findings of G10min group between the two physicians, a senior nuclear medicine physician was consulted to resolve the discrepancy. The accuracy, sensitivity, specificity of the visual diagnosis by the two physicians were then separately calculated across all scan duration groups. For subjective image quality evaluation, each image was rated on a 5-point scale were given (1 = uninterpretable, 2 = poor, 3 = adequate, 4 = good, 5 = excellent) in 3 perspectives: overall quality, noise, and diagnostic confidence. Additionally, 10% percent of the PET images were randomly selected and re-read one month after the initial reading by the two physicians to assess intra-reader agreement.
Image post-processing and objective quantitative analysis
First, all brain T1-MRI images were processed using FreeSurfer v7.4.1 software to conduct cortical parcellations based on the Desikan-Killiany Atlas in native space [28]. Following this, the [18F]florbetapir PET images were co-registered with the corresponding individual T1-MRIs. Region of interest (ROI) masks for four grouped cortical regions (frontal, cingulate, lateral parietal, and lateral temporal) and a composite cortex comprising these regions, along with a reference region mask of the whole cerebellum, were created and applied to the PET images [29]. The SUVr for the composite cortex and the four regional cortical areas was calculated as the mean radioactivity concentration of each ROI normalized to that of the whole cerebellum.
The SUVr value of the composite cortex was used to quantitatively discriminate the binary Aβ status. The best cut-off value was determined by the maximal Yueden’s index via receiver operating characteristic (ROC) analyses for each scan duration group. The corresponding area under the ROC curve (AUC), accuracy, sensitivity, and specificity were calculated to evaluate the quantitative discrimination efficiency. Hedge’s G effect size was reported for the difference between the two groups. Objective PET image quality for each image was quantified using the coefficient of variation (CoV = standard deviation/mean) of the composite cortex.
Statistical analysis
The normality of all quantitative variables was assessed using histograms and the Shapiro-Wilk test. Quantitative variables with a normal distribution were described using mean ± standard deviation and compared between the Aβ-positive and Aβ-negative groups using Student’s t-tests. For quantitative variables without a normal distribution and ordinal categorical variable, data were described using the median and inter-quantile range and compared using the Mann-Whitney U-tests. Nominal variables were summarized by counts and percentages and compared using the Fisher’s exact test. To assess both inter-reader and intra-reader agreement of the subjective visual assessments, the Cohen’s kappa (κ) coefficient and 95% confidence interval (95%CI) were calculated. The image quality evaluation scores on the 5-point scale and coefficient of variation (CoV) between G10min group and other fast scan groups were compared using the Wilcoxon signed-rank test, while the SUVr between them were compared using the paired t-test. Multiple comparison corrections were performed using the Bonferroni method. Bland–Altman analyses were used to assess the potential bias between the composite cortical SUVr of the G10min group and other fast scan groups, with a linear regression line fitted to assess the relationship between the bias and the SUVr value. Statistical significance was defined as P < 0.05. All statistical analysis and the creation of statistical graphs were conducted using SPSS 26.0 (IBM Corporation, Armonk, NY, USA), R 4.1.0 (R Foundation for Statistical Computing, Vienna, Austria) and GraphPad Prism version 9 (Graph-Pad Software, La Jolla, CA, USA).







留言 (0)