
記住我

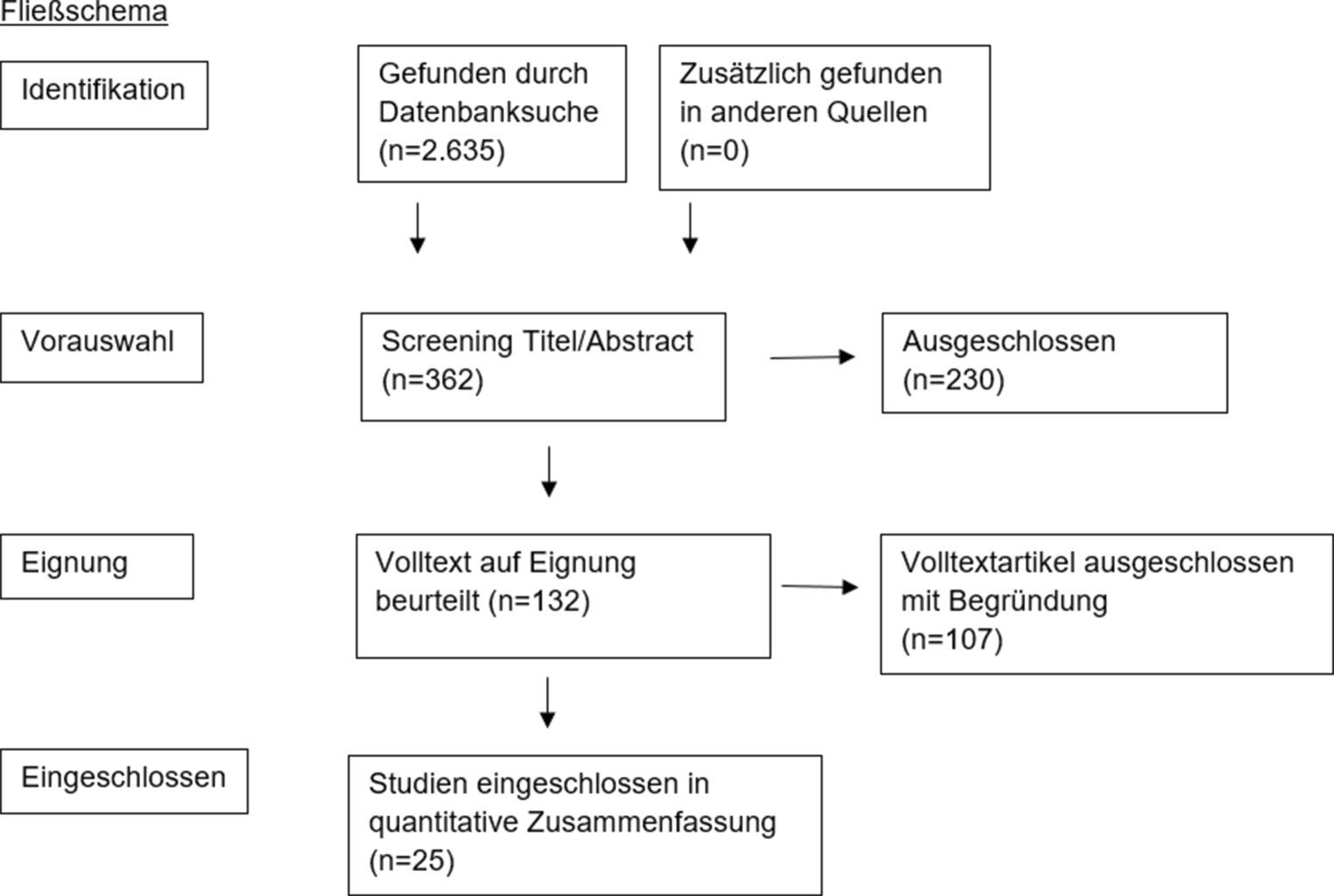

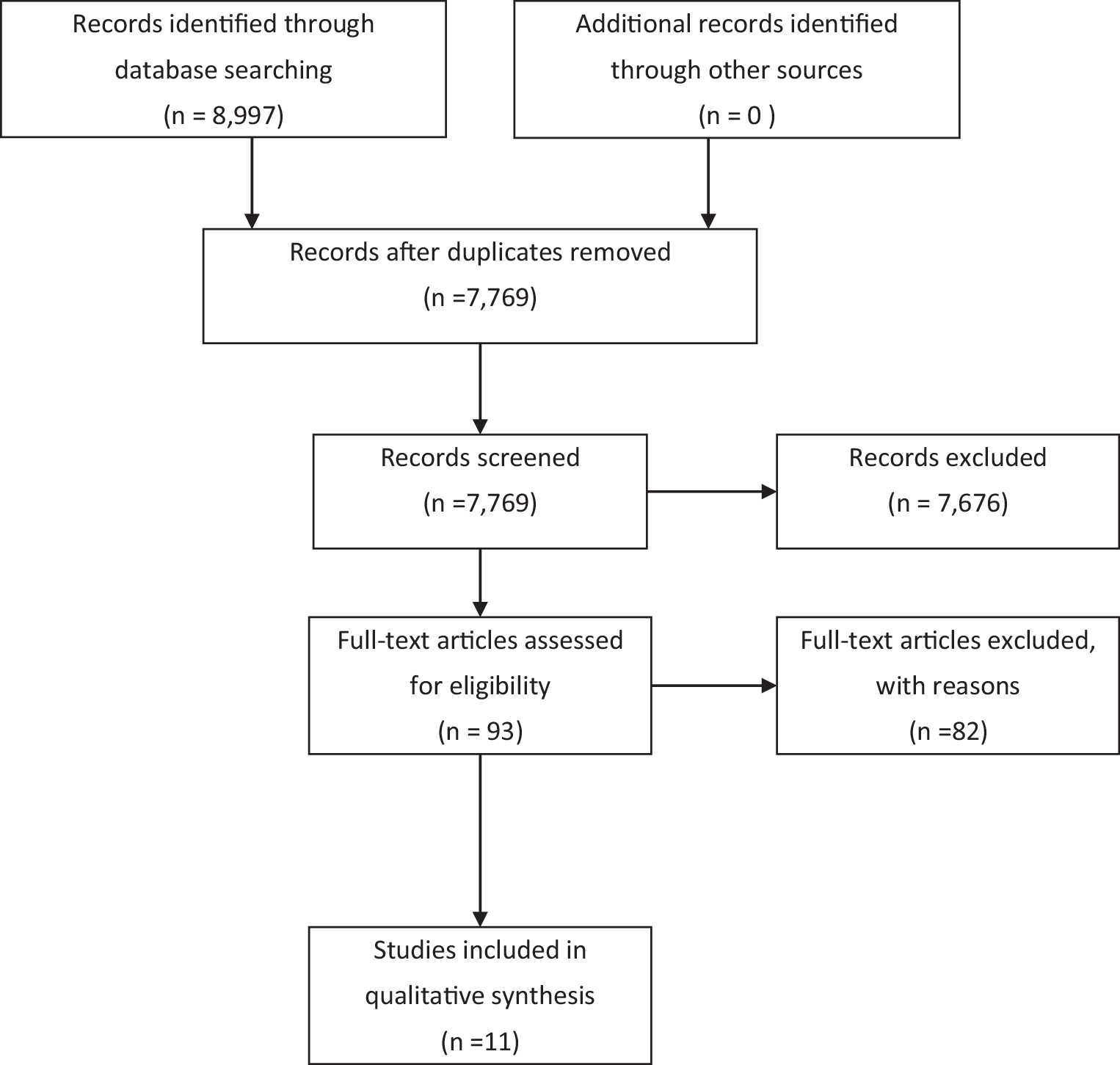
Figure 1 demonstrates an overview of the service landscape. Overall, we identified a broad range of services across Austria with large regional variations. Alongside the prevention–early identification–care/treatment continuum, most services fall under the ‘care/treatment’ category, while we did not identify systematic prevention and universal early detection programs by January 2023. Although some services may be and—according to expert information—are increasingly used by fathers, we did not identify services that explicitly address perinatal mental health problems in fathers or partners, but services predominantly focus on mothers (e.g. by naming them ‘Mutter-Kind-Zentrum’). Except for Vienna, there was no explicit information on whether services were provided in languages other than German and websites describing the services were often restricted to German only.
Fig. 1
Perinatal and infant mental health care services landscape in Austria
Prevention and early detectionIf at all, per January 2023, prevention in the form of education about PMI only took place sporadically or at individual organisations, for example, if there is a personal interest in the topic on the part of the trainer at a course for expecting parents. However, there are many offers where such preventive work could be integrated, for example, as part of the ‘Familienberatungsstellen’ which are provided across Austria, the numerous ‘Eltern-Kind-Zentren’ or women’s counselling services (e.g. ‘Frauenzentrum Osttirol’). Indeed, in the revision of the Austrian national screening program during pregnancy and early childhood (‘Eltern-Kind-Pass’) such counselling is planned to be provided universally, but public information regarding details is missing to date [13].
Regarding screening, universal systematic screening processes covering all women during pregnancy and after birth to detect PMI are neither implemented in any of the nine Austrian states, nor at the national level. Such screening has long been recommended as part of the ‘Eltern-Kind-Pass’ [14]; however, negotiations on whether and how to integrate evidence-based screening tools are still ongoing.
On the regional level, the ‘Wiener Programm für Frauengesundheit’, funded by the Viennese government, has developed screening tools for professionals working in hospital outpatient departments of obstetrics and for gynaecologists and paediatricians working in private practice. In addition, they published a brief general guideline for professionals involved in care during pregnancy and after birth [15]. Similarly, the Styrian health fund has issued a short guidance document [16], however, without stating clear pathways or responsibilities. In general, using such guidance is voluntary, and it is unclear to what extent professionals apply them routinely in a standardised way. Other options for universal screening (after birth) are the midwifery services, whereby mothers are entitled to a defined number of home visits by a midwife for a defined period after birth. Currently, there are no standardised perinatal mental health screening measures in place for those visits, but midwives may address the topic individually. However, only five percent to one quarter of the midwives (depending on the region) have a contract with health insurance [17], meaning that their service is publicly funded.
In contrast to universal screening, a targeted screening is provided by the recently nationwide implemented service ‘Frühe Hilfen’, a low threshold health promotion and/or early intervention approach offered during pregnancy until the child is 3 years old, in case of need for support. Identifying mental health issues is part of their standardised assessment tools. The service also organises referrals to specialised treatment if a need is identified. Yet, families using the service represent only a small subgroup of all annual births.
Care and treatmentWhen the parent is the index patientRegarding care and treatment, we found some form of specialist PIMHC services in each state, yet with substantial disparities across and within states. Regarding hospital-based services (the highest level of care), we identified only one specialised hospital outpatient unit with regular opening hours in Vienna as of January 2023. In some cases (Wels), existing units had to be closed due to a lack of resources. In others (Tyrol, Styria) the foundation of units is planned or in the process of implementation. Sporadically, there are small-scale offers with restricted opening hours available (e.g. Klagenfurt hospital).
Furthermore, there are nine to ten formal inpatient mother–baby beds available in three Austrian states (Vienna: 4; Styria: 2; Upper Austria: 3 to 4). Four states have an option to admit mothers with their baby in an emergency (Lower Austria, Salzburg, Vorarlberg, Upper Austria), yet without permanent infrastructure and established perinatal mental health care teams. Three states (Tyrol, Carinthia, Burgenland) have no options to admit mothers with their babies. There are currently no specialised hospital daycare facilities or other forms of acute specialised treatment (e.g. home treatment) available. According to expert information, the number of mother–baby units is planned to be slightly increased in some states (e.g. in Salzburg/Schwarzenberg Klinikum).
Experts informed us that admission into all types of mother–baby units in adult mental health care facilities is usually subject to the mother still being able to care for the child. Professional care for infants is provided but organised differently, for example, by permanently employed or liaise infant nurses or by psychiatric nurses trained in infant care. Details on treatment approaches are not published on the hospitals’ websites. We, therefore, do not know to what extent special offers to address the mother–child interaction are available or whether mothers primarily receive routine adult mental health treatment and children are co-admitted, guaranteeing custody and childcare. If the mother’s mental health makes her unable to care for the infant, partners or other potential carers are asked to take custody. The infant may be admitted to the paediatric unit without such a carer. Mother–infant interaction programs are not possible in this situation.
On a lower level of care, we identified a variety of specialised psychotherapy and attachment-oriented services in the community setting. Examples of those are therapeutic offers for mothers with mental health problems in Tyrol and Vienna as part of the ‘Frühe Hilfen’ service, infant–parent psychotherapy services offered by specialised organisations (e.g. ‘Österreichische Gesellschaft für Kinder- und Jugendpsychotherapie’) or by therapists in private practices, and attachment-oriented therapies. The latter can be specific forms of therapy (e.g. body-oriented therapy) or counselling (emotion-oriented) or may also include parenting skill training and support in daily life. Examples of services are ‘Grow Together’ offered in Vienna or ‘Zoi’ provided in Tyrol. In one state (Salzburg), programs designed to support parents with a mental illness offer a scheme for the perinatal period (‘Verein Jojo’) or extend their target groups to include parents in the perinatal period (‘PrEKIDS’). As a low threshold service in case of mild symptoms, ‘Frühe Hilfen’ has been available across all states since 2023. This is also one of the few services which offer outreach care in the families’ homes.
In addition to specialist services, services are available that may be used by parents with a mental health problem in the perinatal period but that do not treat the health issue and/or do not have specially trained staff. These include general adult mental healthcare facilities and services, including pharmacological treatment and psychiatric/psychological consultation and liaison service (e.g. to support the obstetrics departments in case of a mother’s mental health problem during admission around birth). Some professionals working in those services may have special training or experience in treating PMI. However, this qualification is not publicly documented. Furthermore, several services in the social sector, most notably those provided by the child and youth welfare as part of the ‘Unterstützung der Erziehung’-scheme (e.g. ‘Sozialpädagogische Familienbetreuung’), are used to some extent by parents with a PMI. Often, their use is mandatory and subject to severe problems and referral from the child and youth welfare. Such services may ensure that the parent receives treatment elsewhere but focus on supporting parenting and avoiding child neglect.
When the infant is the index patientRegarding specialised care where the infant is the index patient, we identified hospital outpatient units (e.g. for babies with excessive crying) and day-clinics for infant psychosomatic care (e.g. ‘Baby-Care-Ambulanz’ at the ‘Klinik Favoriten’ in Vienna) in five of the nine Austrian states (Salzburg, Tyrol, Upper Austria, Vienna, Vorarlberg). In some regions, infants with psychosomatic or mental health symptoms can be admitted to a paediatric or child and adolescent mental health care unit in hospitals with a parent (e.g. Hall in Tirol with six beds), but not if the parent has severe mental health symptoms.
Informal supportWe identified self-help groups with a focus on PMI in three Austrian regions (Styria, Tyrol, Vienna) on the websites of self-help associations: the drop-in ‘Selbsthilfegruppe für Mütter mit psychischen Belastungen nach der Geburt’ in Innsbruck, the Styrian group ‘postpartale Depression’ and the Viennese group ‘Mutterglück! Mutterglück?’ organised by ‘NANAYA (Zentrum für Schwangerschaft, Geburt und Leben)’. They meet once to twice per month, can be accessed free of charge, and two of them are supported by professionals.
Service characteristicsProvidersThe services are provided by a mix of public and private providers, whereby private providers outweigh the number of public providers. Public providers are mostly restricted to hospital-based services, whereas programs in other settings are generally offered by private providers. All private providers are nonprofit organisations.
The size of organisations in terms of service portfolio and geographical coverage varies, ranging from small organisations providing a service in a single district, to larger ones providing a greater variety of services and/or serving a larger geographical area. An example of the former is the organisation ‘ZOI’ in Tyrol, which primarily offers services to improve parent–infant attachment in one Tyrolean district (Kufstein). An organisation representing the latter is ‘Beratungsstellen ÖKIDS’, organised by the Austrian Society for Child and Adolescent Psychotherapy, which offers infant–parent psychotherapy in five states. Most organisations are based in one of the nine Austrian states.
FundingWith few exceptions (‘Eltern-Kind Pass’, ‘Frühe Hilfen’, ‘Familienberatung’), which are funded and governed at the national level, and some health insurance-funded outpatient services (midwifery support after birth), responsibility for the funding of most of the services identified rests with the regional governments and sometimes even with districts or city governments. Consequently, various funding sources and all types of public payers, funding health and social care services in Austria, are involved. It is noticeable that some programs offered within hospitals (usually outpatient services) are not funded via the regular hospital outpatient reimbursement scheme, but via separate funding arrangements, sometimes involving many sources, including project-based funding. Examples are the hospital outpatient units ‘FEM’ and ‘FEM Süd’ in Vienna, which are funded by at least five different sources (e.g. ‘Stadt Wien’, ‘Wiener Institut für Gesundheitsförderung’, ‘Österreichische Gesundheitskasse’).
In addition to public funding, private funding plays a role. Firstly, some services are in parts and, in rare cases, funded fully from donations from regional companies, charity organisations, or private donors (e.g. ‘Verein JoJo’ in Salzburg). Secondly, users must pay private fees or co-payments for some services to access them (e.g. prescription fee). However, in case of user charges, fees may depend on the economic situation of the user, and if required, services may be offered free of charge. Services for which up to full private payment can be required most often are psychotherapy services, except if they are provided under a contractual arrangement with a public funder (e.g. health insurance) or by an organisation which is publicly funded and provides psychotherapy by employed therapists.
Reimbursement schemes of providers, which are publicly funded, differ considerably across services and regions. Hospital inpatient services are funded via a diagnosis-related group (DRG) system, where interventions requiring specific resources are usually linked to a defined tariff covering costs. Yet, there is no specific reimbursement code for mother–child admissions in adult mental health care units. Hospital owners with mother–baby beds deal differently with this situation. Some have arranged to reimburse admission using a code from child and adolescent mental health admissions (‘Einheiten mit der Behandlungsform E/Eltern-Kind’). However, this code was abolished in 2021. Others use the standard DRGs from adult mental health to reimburse the costs for treating the mother, and the baby is coded as an ‘accompanying person’.
Outpatient services in private practices in the health care sector (e.g. outpatient psychiatrists, psychotherapists, midwives) are reimbursed via a tariff per service negotiated between the professional groups and the health insurance. In some cases, reimbursement is a mix of flat rates and tariffs per service. Reimbursement for organisations in the social sector which receive public funding varies. Some organisations have short- or long-term contractual arrangements (e.g. those funded by child and youth welfare), while others may receive subsidies or funding on a project basis. These arrangements are subject to the payer’s budgetary situation and the decision maker’s discretion. They are, therefore, linked to less financial security for providers than services funded via hospital funding schemes or health insurance tariffs.
Professional groups involvedMultiprofessional teams characterise the workforce in most of the services identified. Providers mentioned more than 40 professional groups or auxiliary staff on their websites. These include medical specialities (e.g. psychiatrists, gynaecologists), allied health professionals (e.g. nurses, midwives, psychologists, different types of therapists), pedagogues and educational specialists (e.g. social pedagogues), social workers, counsellors with diverse backgrounds and several allied professionals and auxiliary staff (e.g. life coaches, interpreters). Professional groups stated most often were psychologists and psychotherapists.
Coordination and interdisciplinary exchangeAccording to the Austrian depression report [14], formal exchange between services and professional groups currently exists in Vienna. The network ‘Psychosoziale Gesundheit in der Schwangerschaft’ meets two to three times per year, aiming to improve PIMHC (including identifying gaps) and foster interdisciplinary training and exchange. Vienna has also established semi-formal referral pathways for professionals identifying a parent with a PMI, whereby the outpatient perinatal mental health unit plays a crucial role in diagnostics and assessment and arranging further treatment and care according to the parents’ needs. We have not identified similar initiatives in the other eight states.
留言 (0)