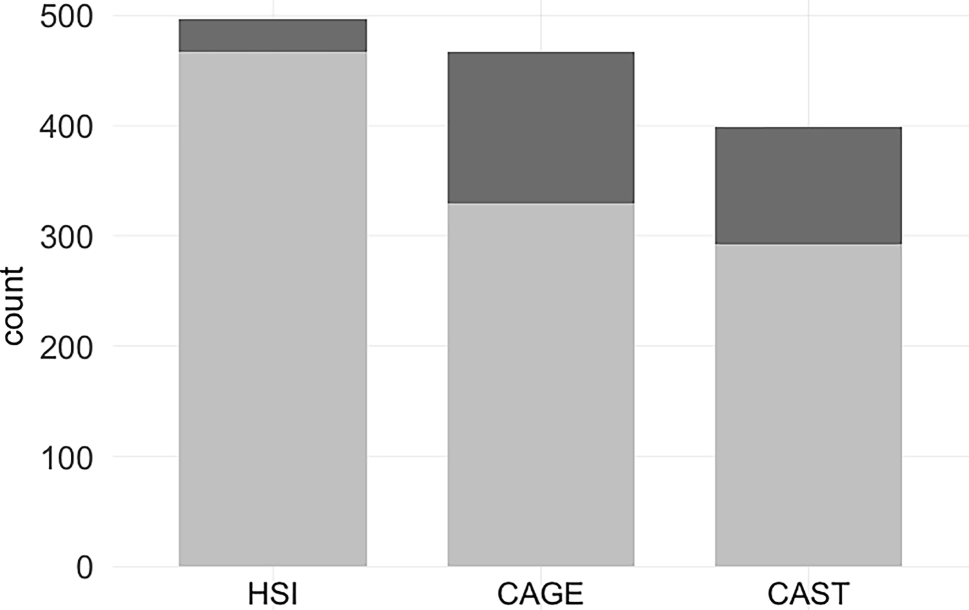
Patient demographics and baseline characteristics are outlined in Table 1. The majority of the sample (84.2%) were diagnosed with AN restrictive subtype. Among the participants, 36.8% scored above the cut-off of 6 on the AQ-10 and were classified as HAT patients, with 55.3% classified as LAT patients. The majority of patients (76.3%) displayed severe impairment in work and social functioning, as assessed by the WSAS (scoring above the threshold of 20).
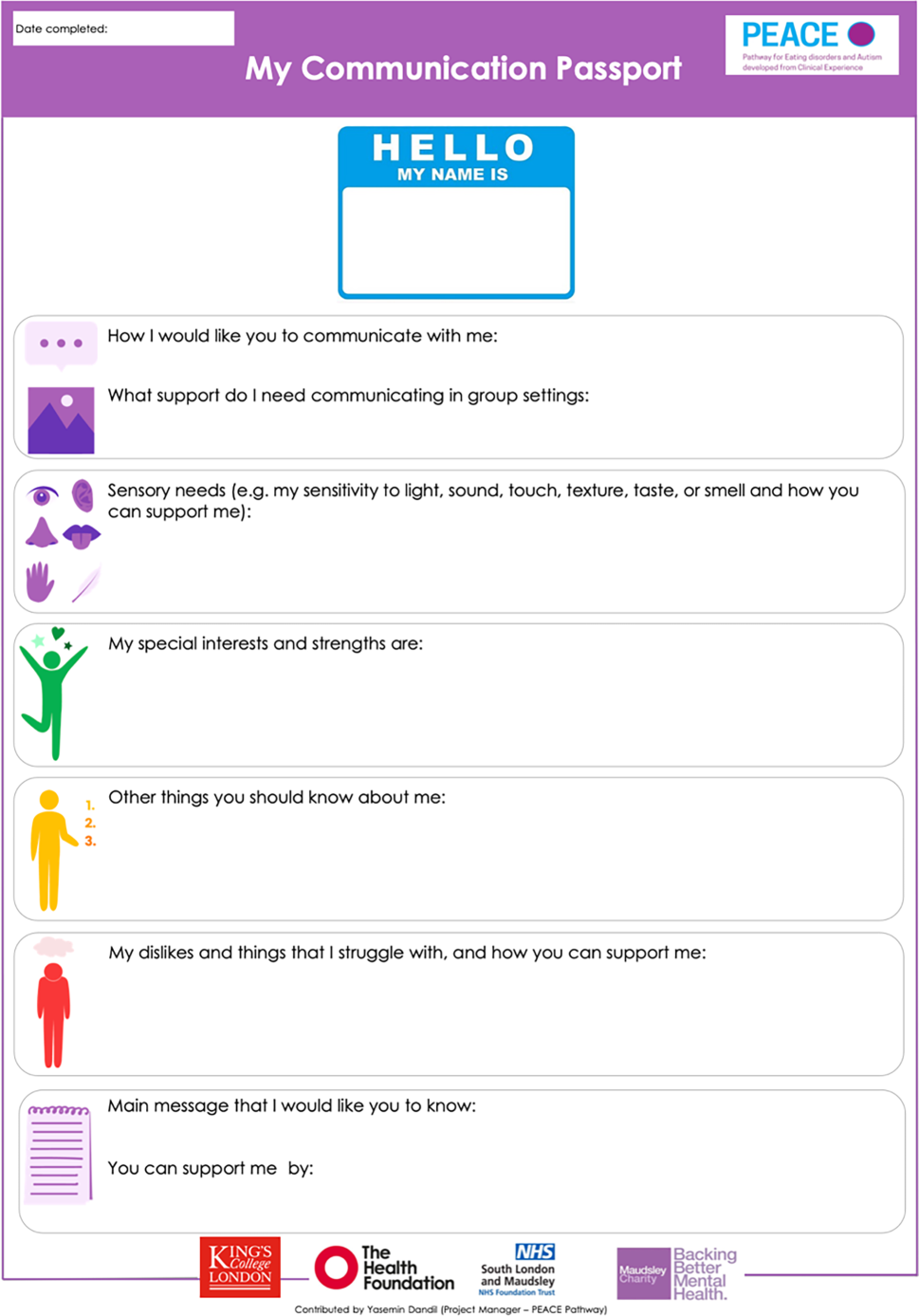
The examination of the entries in the communication passport revealed a range of valuable patient insights, summarised in Table 2. These included their communication preferences, sensory difficulties and needs, special interests and personal strengths, important messages about personal values intended for the care team, struggles and dislikes, and different kinds of support required. We discuss each aspect individually in the following sections, providing a more comprehensive understanding.
Communication preferences
Patients reported their communication preferences in response to the first question on the communication passport: “How I would like you to communicate with me.” Analysis revealed two predominant themes: patients’ preferred mode of communication, and their preferred tone and style of communication. Regarding their preferred mode of communication, patients highlighted the importance of private, one-on-one conversations away from distractions. When necessary, non-verbal ways of communication such as written materials, visuals, and body language were also helpful. Furthermore, they expressed a need for patience, requesting that information be repeated multiple times to ensure understanding.
Regarding the preferred style and tone of communication, many patients highlighted the importance of kind and gentle communication that is delivered “calmly, kindly, gently” with a “soft voice”. Moreover, patients value transparency and honesty, preferring open and direct conversations regarding their treatment rather than leaving things unsaid or concealed from them. Patients with and without autistic traits gave largely similar responses in this domain. However, only HAT patients mentioned a requirement for information to be reiterated multiple times.
Sensory sensitivities
Various domains of sensory sensitivities were identified in patients’ response to the prompt “Sensory needs (e.g. my sensitivity to light, sound, touch, texture, taste, or smell and how you can support me)”, including auditory, olfactory, tactile, visual sensitivities, as well as sensitivities to taste and texture of food. Auditory sensitivities were prevalent among the majority of patients, who found noisy environments such as “slamming doors”, “alarms”, “footsteps”, and “loud music on the radio” stressful, although some patients preferred background noise. Following auditory sensitivities, tactile sensitivities were commonly reported, with responses divided into sensory-seeking behaviours, such as the need for stress balls and fidget toys, and sensory-avoidant behaviours, such as discomfort with physical contact like hugging. Additionally, many patients reported sensitivities to bright or flashing lights (“Low light helps me focus. Bright lights are distracting”), strong smells such as perfumes, and preferences regarding taste and texture of food, with some preferring plain and bland foods while others favoured strong tastes (“need flavour and need sweet”). Overall, both HAT and LAT patients reported various sensory sensitivities.
Special interests and strengths
In response to the prompt “My special interests and strengths are. . .”, patients reported a wide range of interests, which were categorised into: cooking and baking; entertainment and leisure (e.g. favourite TV shows and films, traveling, games, shopping); education and childcare; intellectual pursuits such as reading, science and maths; music and performing arts; nature and animals; religion; sports; and visual arts and crafts. Patients also reported their strengths, categorised into personality-related strengths (such as truthfulness, integrity, willingness to help others, and curiosity) and skill-related strengths (such as communication skills and analytical skills). Both HAT and LAT patients reported a wide range of special interests and strengths with no difference between the two groups.
Important message to the care team
Patients also used the space for “Other things you should know about me” and “Main message that I would like you to know” to convey significant messages to the care team: firstly, the importance of their personal relationships with family, friends, and pets (“My family and friends all mean a lot to me”); secondly, the significance of their personal identity (“Treat me like a normal person”; “Don’t talk to me like I am an illness”) and cultural identity (including their hometown, preferred pronouns, and autism diagnosis); and thirdly, their determination to improve with treatment (“I want to get better”). Patients with and without autistic traits gave similar responses.
Dislikes and struggles
In response to “My dislikes and things that I struggle with”, patients reported their dislikes and struggles across five areas: adapting to changes and managing information overload (“[Dislike] schedule that is uncertain”; “[Struggle with] processing information”); expressing needs and emotions (“I struggle to ask for help”); imposed control and patronisation from others (“I don’t like being forced”: “[Dislike] being patronised”); low self-esteem and self-compassion (“[Struggle with] giving myself permission for enjoyable activities”); and navigating social attention and interaction (“Hate being in the spotlight”; “Find it hard to open up to people”). Notably, only HAT patients and none of the LAT patients reported difficulties with changes and information overload.
Support needed
Several questions on the communication passport prompted patients to outline the kinds of support they require (e.g. “What support do I need communicating in group settings”; “My dislikes and things that I struggle with, and how you can support me”; “You can support me by”). From their responses, seven key support needs were identified. Firstly, patients expressed a need for support with group participation. This involved being invited in during discussions and given the opportunity to contribute and receiving individual check-ins after the group. Patients also reported a need for reassurance and external permission to eat from the care team (“The reassurance that it is okay to eat my meals”). Additionally, they valued receiving advanced warning about any changes to plans (“If a plan is going to change, please tell me”). Furthermore, patients appreciated the care team checking in on their well-being (“Check in with me”; “Asking me what could help in the moment”). They also appreciated conversations on topics unrelated to their illness (“Help by talking about other things outside of [ED]”). Lastly, patients stressed the importance of having personal space and time alone (“I need time on my own”) and expressed a desire to be involved in decisions regarding their treatment and care (“Keep me in the loop”; “Be collaborative with me”). Overall, patients with HAT and LAT reported similar support needs.



留言 (0)