
記住我


The study is a university-based, single-center, retrospective data analysis. Data were derived from patients of the Neurological Department of the Medical University of Vienna from the period August 1998 to October 2021. Patient-related data of the deceased patients were obtained from the Research, Documentation, and Analysis (RDA) system of the Medical University of Vienna. Data of deceased patients up to March, 14th 2022 were accessed according to the records of the RDA and the Allgemeines Krankenhaus Information Management system (AKIM).
ParticipantsParticipants underwent a complete medical and neurological examination at the Department of Neurology. Individuals were included in the study if they were examined both for depression and dementia. Patients were divided into three subgroups of cognitive impairment, according to the precursors of Alzheimer’s dementia: SCD, naMCI, and aMCI. Patients without cognitive decline or a severe form such as Alzheimer’s dementia, evidence of stroke, traumatic head injury, and psychiatric syndromes (e.g. schizophrenia, severe anxiety disorders such as Bipolar Disorder, severe Personality Disorders such as Borderline Disorder, severe compulsive disorders) causing pseudo-dementia were excluded from the study. Exclusion criteria were assessed via clinical exploratory interview.
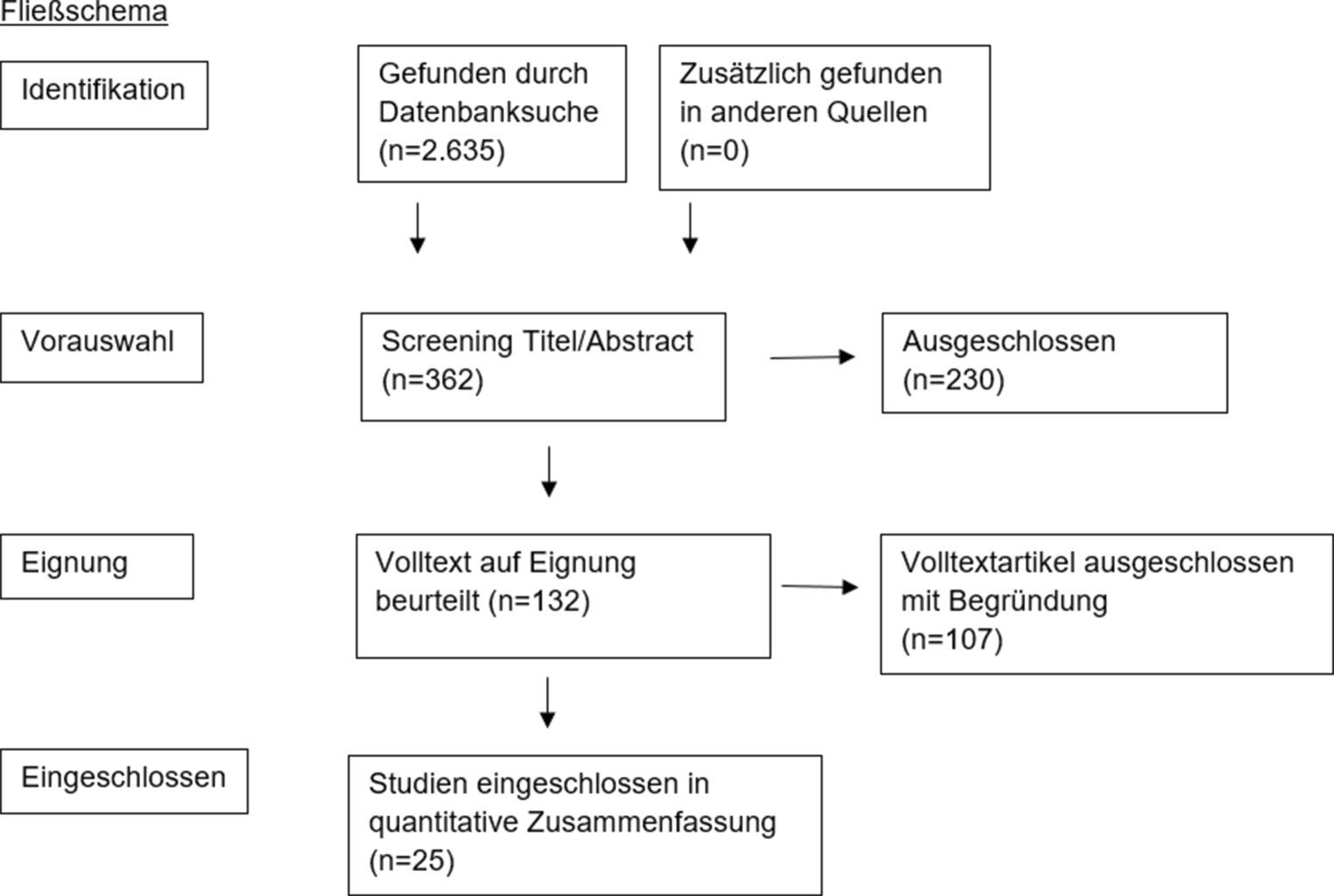
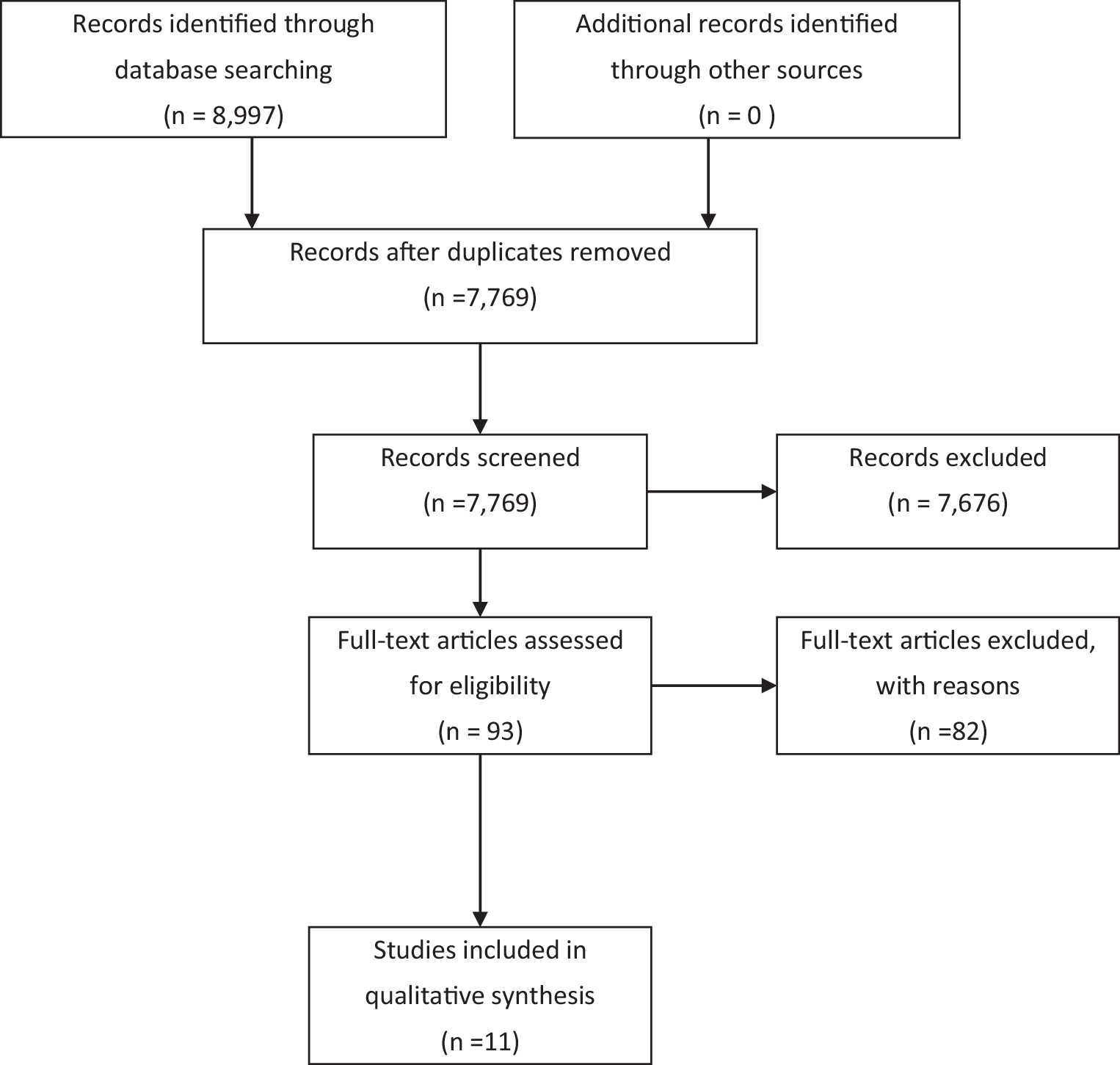
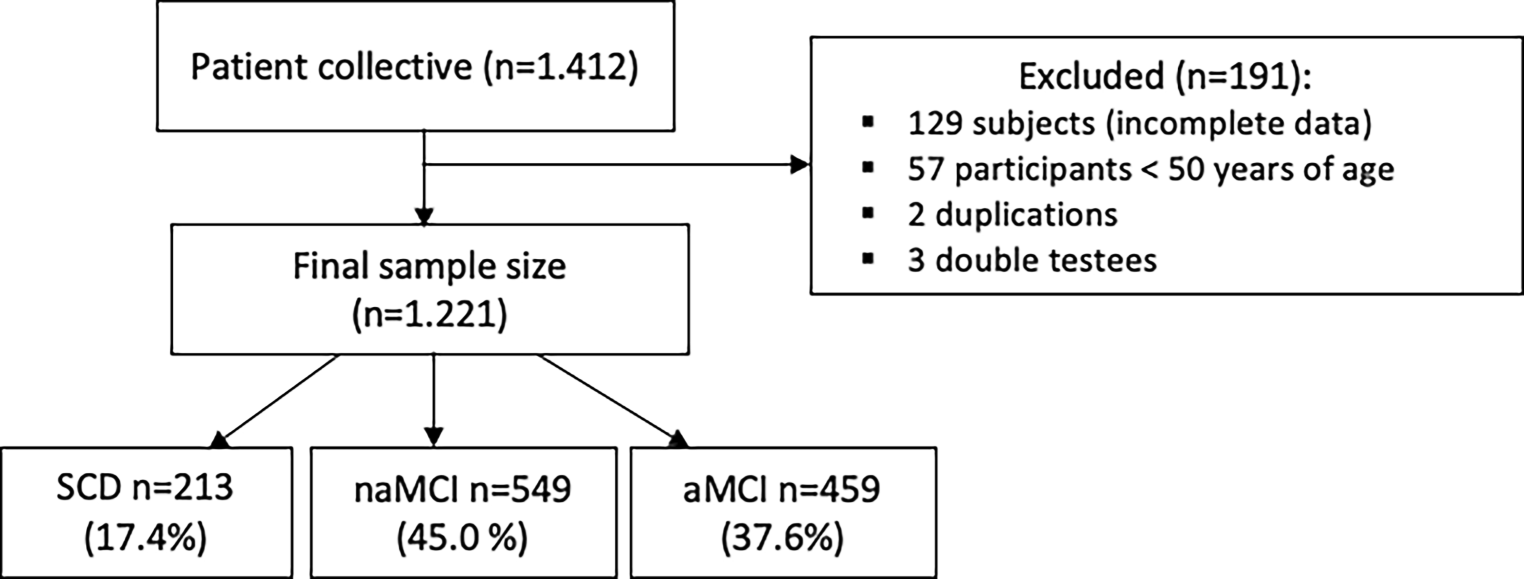
The diagnosis of SCD was made according to the classification of Jessen et al. based on self-reported concerns of cognitive problems. Individuals affected with SCD were not diagnosed until 1999 [16]. Similarly, Petersen’s criteria were applied to diagnose MCI patients [3]. Sociodemographic characteristics about age, gender, and average school attendance in years were considered. Neuropsychological abilities indicated by the Mini-Mental-State-Examination (MMSE), vocabulary test (WST-IQ) and the Neuropsychological Test Battery Vienna (NTBV) were used. The neuropsychological testing as well as the assessment of depressiveness by Beck Depression Inventory (BDI-II) and Geriatric Depression Scale (GDS-15) were conducted on the same day. Figure 1 illustrates the exclusion protocol for participants who did not meet the required criteria for the present study. With a total of 1221 cases, the sample was divided into 213 SCD, 549 naMCI, and 459 aMCI patients. The age range was between 50–90 years, as most of the memory clinic’s patients with cognitive decline belong to this age group. The study was approved by the ethics committee of the Medical University of Vienna (2193/2021) and followed the tenants of the Declaration of Helsinki.
Fig. 1
Flowchart, showing the selection of the patient collective based on the exclusion of cases from the study and the distribution of the remaining patients. SCD subjective cognitive decline, naMCI non-amnestic mild cognitive impairment, aMCI amnestic mild cognitive impairment
InstrumentsDepressive symptomsThe Beck Depression Inventory (BDI-II) assesses the severity of depressive symptoms in a clinical setting. The BDI-II consists of 21 items, operationalizing sadness, pessimism, feelings of failure, loss of joy, feelings of guilt, feelings of punishment, self-rejection, self-reproach, suicidal thoughts, crying, restlessness, loss of interest, inability to make decisions, worthlessness, loss of energy, change of sleeping habits, irritability, change in appetite, difficulty concentrating, fatigue or exhaustion, and loss of sexual interest, based on a four-staged rating [17, 18]. The scoring range is as follows [19] < 13: no depression or clinically unremarkable or remitted; 13–19: mild depressive syndrome; 20–28: moderate depressive syndrome; ≥ 29: major depressive syndrome.
The Geriatric Depression Scale (GDS-15) is a widely used international assessment tool that provides reproducible information about the mental state of ageing patients. The 15 questions are answered with yes/no. The following scores are obtained after counting positively answered questions [20] 0–5 points: inconspicuous; 5–10 points: mild to moderate depression; 10–15 points: severe depression.
Neurocognitive statusNeurocognitive tests were used to determine the progression of the patient’s neurodegenerative processes. The Mini-Mental State Examination (MMSE), a brief assessment of cognitive performance, is often used as part of the screening and diagnosis of potential dementia [21]. It contains few items on episodic and semantic memory or spatial-visual reasoning and does not test executive function. Performance is impaired by age, ethnicity, and low educational level [22]. The Wortschatztest (WST/WST-IQ) provides a rapid assessment of verbal intelligence level and language comprehension. The average IQ value is between 85 and 115 IQ points (μ = 100, σ = 15) [23]. The Neuropsychological Test Battery Vienna (NTBV) is a standardized neuropsychological test series for the assessment of objective cognitive impairment and dementia. The inventory includes categories such as psychomotor speed, attention, language, memory, and executive functions. These areas of cognitive function are characteristically affected in Alzheimer’s dementia [24]. In the present study, 24 subtests of the NTBV were addressed in six domains. The NTBV can be obtained from www.psimistri.com [25].
Statistical analysisFor the realization of the descriptive and inferential statistical analyses, IBM SPSS® 28.0 for macOS was used. The hypotheses testing was implemented under the assumption of an alpha level of 5% (α = 0.05), according to the Type-I-Error. The results in p ≤ 0.05 were considered significant in the analyses. All the statistical procedures were performed two-tailed. In the case of multiple testing, Bonferroni adjustment was considered to avoid the accumulation of type I errors.
For the characterization of metric parameters, mean (M) and standard deviation (SD), a range of minimum (min) and maximum (max) were used as key values. In case of skewed data distribution, the median (Md) and interquartile range (IQR, PR 25–75%) were assessed and reported. 95%-confidence intervals (CI) were generated specifying a range estimate [26]. For the description of nominal scaled parameters, the frequencies (n) and the proportional values (%) were calculated and displayed. In the inferential statistics section, variance analytic procedures (ANOVA) were calculated to test for differences in metric, at least interval-scaled, parameters between more than two groups [27]. In addition, the homogeneity of variances had to be considered, which was examined by Levene’s test. In presence of heterogeneous variances, Welch’s ANOVA was applied [28]. Non-parametric analyses, Mann-Whitney’s U‑testing, and the Kruskal-Wallis-Test were used for at least ordinally scaled data comparing independent groups [27]. The relationship between two nominally scaled variables was examined based on cross-tabulations using chi-square testing. The relationship between two metric, at least interval-scaled variables was calculated using Pearson’s coefficient r. For skewed variables, Spearman’s parameter-free rank correlation rs was also applied [26].
Furthermore, the Kaplan-Meier function and the post-hoc log-rank procedure were applied to analyze the differences in survival among the different diagnosis groups [29]. The Cox Proportional Hazards model was used to evaluate the weight of depressive symptoms in predicting the mortality of patients with cognitive decline considering the time component; follow-up time until death and excluded cases. The hazard ratio (HR) was reported as a measure of the relative risk of a predictor. The influence of the severity of cognitive decline as well as the impact of covariates on the mortality of the patients was determined [30, 31]. These covariates were included hierarchically block-wise in five steps, to successively explain the additional value considering the added predictors using the so-called enter method per block [30]. In the 1st block, the depression scorings (BDI-II, GDS); in the 2nd block the sociodemographic covariates age (years), gender (0) male, (1) female; in the 3rd block education in years and WST-IQ were used; in the 4th block the diagnostic subgroups considering SCD as reference level; and finally in the 5th block the z-standardized factor scores of the six NTBV dimensions. Achieving a dimensional reduction and overview, the NTBV subtests were subject to a principal component analysis (PCA) with subsequent orthogonal rotation (varimax approach according to Kaiser) [32]. To fully assess the information content of the items, so-called factor scores were generated. The main advantages of this process are z-standardized scores (μ = 0, σ = 1) with perfect independence (r = 0) and complete uncorrelatedness of the factor scores [33,34,35].
留言 (0)