Participants
Two-hundred-and-two healthy adults (18–59 years of age) without psychiatric illness were studied at the U.S. National Institutes of Health (NIH) Clinical Center. Of these, 187 participated in [18F]-FDOPA neuroimaging to measure presynaptic dopamine synthesis capacity (98 [52.4%] female, mean age 35.7 ± 11.1 years), and 104 participated in [18F]-fallypride neuroimaging to measure dopamine D2/3 receptor availability (47 [45.2%] female, mean age 38.1 ± 11.1 years). All participants were of European decent and were free of psychiatric diagnosis, neurological condition, substance use disorder or other confounding medical conditions as determined by clinical evaluations, including history and physical examination, psychiatric diagnostic interview [16], laboratory testing, and clinical magnetic resonance neuroimaging.
Genetics
Genotyping, quality control, and imputation procedures were conducted as previously reported [17]. Participants provided peripheral venous blood samples, and DNA from mononuclear cells was extracted for genotyping, which was conducted with Illumina BeadChips (510K–2.5 M SNP chips). Quality control was performed in standard fashion with all samples demonstrating SNP missingness <0.05 (before sample removal); subject missingness <0.02; autosomal heterozygosity deviation (|Fhet|<+/−3.5 standard deviations); SNP missingness <0.02 (after sample removal), SNP Hardy-Weinberg equilibrium (HWE) p > 10−6; minor allele frequency (MAF) > 0.01; and identity by descendent threshold of 0.185. Data were phased using Shapeit software (https://mathgen.stats.ox.ac.uk/genetics_software/shapeit/shapeit.html), and imputation used IMPUTE2 (https://mathgen.stats.ox.ac.uk/impute/impute_v2.html) with default parameters and a chunk size of 250 Kb. The 1000 Genomes Phase 3 data were used as a reference panel for the Illumina HumanOmni2.5-v1.2 chip, and the resultant imputation served as the reference panel for the remaining smaller chips. The genomic data were subjected to principal component analysis using PLINK software (https://www.cog-genomics.org/plink/1.9) with the first three components retained for use as population stratification covariates.
Polygenic scores both for unselected schizophrenia (non-TRS) risk and for differential TRS risk relied upon summary statistics derived from two recent, large-scale genetic association studies: the Psychiatric Genomics Consortium “Wave 3” schizophrenia genome-wide association study meta-analysis [18] and the treatment-resistance interaction meta-analysis of Pardiñas and colleagues, which evaluated cohorts of individuals who had been prescribed clozapine and had evidence for failure of at least 2 other antipsychotic medications [14]. PRSice-2 software (https://choishingwan.github.io/PRSice/) was employed to calculate polygenic risk scores both for non-TRS and for TRS at multiple p-value thresholds (ranging from 5 × 10−8 to 1.0), which were then reduced using principal components analysis with R software (https://www.r-project.org/), as previously described [19]. Resultant primary (first component) summary measures of risk proclivity for non-TRS and TRS were then forwarded for further analysis.
NeuroimagingAcquisition procedures
All scans were performed after a four-hour minimum abstinence period from caffeine and nicotine. Additionally, for [18F]-FDOPA scans, a six-hour minimum fast (to prevent amino acid-mediated competition for tracer transport across the blood brain barrier) was required, and participants were administered carbidopa 200 mg by mouth approximately one hour prior to [18F]-FDOPA injection (to prevent peripheral tracer decarboxylation). For [18F]-FDOPA scans, a General Electric Advance PET camera was used in 3D mode. An individualized thermoplastic mask was contoured to each participant’s head to limit movement. After head position was established in the camera bore, a 68Ge transmission scan for attenuation correction was performed. [18F]-FDOPA emission scans immediately followed bolus tracer injection (target dosing of up to 16 mCi; mean dose 15.3 ± 2 mCi; mean specific activity 1180 ± 393 mCi/mmol) and were collected in dynamically binned frames over approximately 90 min.
All [18F]-fallypride scans were carried out on a Siemens ECAT HRRT camera outfitted with a Northern Digital Polaris Vicra optical measurement system. Prior to scanning, participants donned a cap with attached spherical reflectors, which permitted head motion tracking. After head position was established in the camera bore, a 137Cs transmission scan for attenuation correction was performed. [18F]-fallypride emission scans began immediately following bolus tracer injection (target dosing of up to 5 mCi; mean dose 5.1 ± 0.2 mCi; mean specific activity 2603 ± 1249 mCi/μmol) and were collected over a period of approximately four hours, which included two brief planned breaks for the participant out of the scanner. Re-positioning and transmission scanning preceded emission scanning upon the participant’s return to the gantry following each break.
In separate imaging sessions, participants underwent T1-weighted structural magnetic resonance imaging (MRI) at 3T for coregistration and spatial warping purposes.
Data processing procedures
For [18F]-FDOPA scans, reconstruction with filtered back-projection with registered attenuation correction that adjusted for frame-wise head motion was performed. For [18F]-fallypride scans, reconstruction with ordered subset expectation maximization was conducted, with head tracking data used to correct for motion.
Each participant’s T1-weighted structural MRI volumes were averaged, intensity normalized [20] and segmented using Freesurfer (https://surfer.nmr.mgh.harvard.edu/) and AFNI (https://afni.nimh.nih.gov/) software tools. MRI scans and segmentations were manually checked for quality and any segmentation errors hand edited. A centroinferior gray matter cerebellar region that excluded vermis to limit specific binding as well as lateral/superior parasinus regions was used to define a reference region for use in modeling for both ligands.
Using FLIRT software (http://fsl.fmrib.ox.ac.uk/fsl/), each dynamically binned PET frame was rigid-body aligned to a central reference frame in the series to further address interframe head motion. Because of the shorter frame duration and limited anatomical definition in the first three PET frames, these frames were yoked to the fourth frame during this alignment step. Using SPM software (https://www.fil.ion.ucl.ac.uk/spm/software/), anatomical MRI volumes and segmentation maps were coregistered to the series mean PET volume. This allowed delineation of time-activity curves for average activity in the cerebellar reference region, which served as an input function to subsequent modeling and were visually inspected to ensure adequate quality for all subjects. ANTS software (http://stnava.github.io/ANTs/) was employed to conduct spatial warping of MRI volumes (and coregistered PET data) to a standard, MNI space template, and smoothing with a 10 mm Gaussian kernel was achieved with SPM software to improve signal to noise ratios.
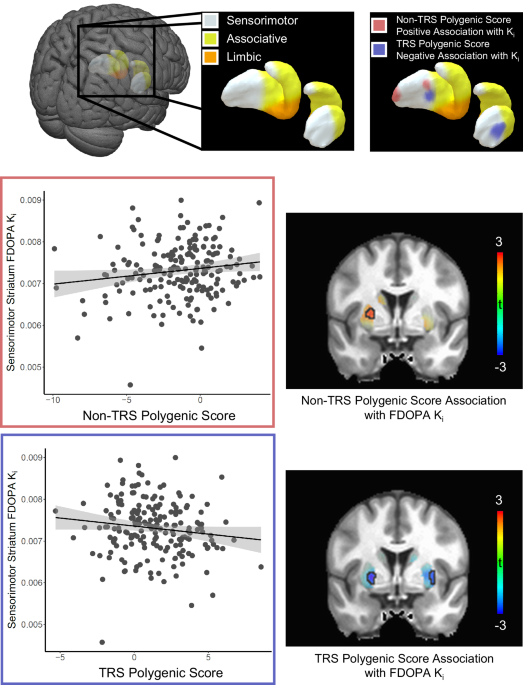
For primary analyses of [18F]-FDOPA data, the tracer specific uptake rate constant, Ki, a measure of presynaptic dopamine synthesis capacity, was estimated voxelwise across the striatum with PMOD software (https://www.pmod.com/web/) using the non-invasive graphical linearization approach, which assumes an irreversible component (in this case, tracer engagement with DOPA decarboxylase and [18F]-fluorodopamine accumulation) over the course of the scan [21]. The whole striatum was delineated for primary analyses as well as segmented into three bilateral canonical functional subregions (associative, sensorimotor, ventral) as previously described [22], and average Ki was calculated for each subregion in addition to the whole striatum.
Following evidence suggesting thalamic D2/3 dopamine receptor availability is lower in schizophrenia [15], for [18F]-fallypride data, the binding potential estimate, BPND, a measure of D2/3 dopamine receptor availability, was calculated voxelwise across the thalamus as well as the striatum using the simplified reference tissue model as implemented in PMOD [23, 24]. The whole thalamus was delineated for initial analyses and subsequently segmented into seven bilateral subregions reflecting distinct nuclei groups [25]: anterior; ventral anterior group; medio-dorsal group; ventral latero-ventral group; ventral latero-dorsal group; pulvinar; and a cluster enclosing the central lateral, the lateral posterior and the medial pulvinar (CLLPMP) [25], with mean BPND calculated for whole thalamus and its subregions. Additionally, average [18F]-fallypride BPND for whole striatum and striatal subregions as defined above were also calculated.
Statistical analyses
Associations between striatal Ki and polygenic predictor variables were tested using linear modeling in R software, with nuisance covariates for age, sex, and population stratification. Separate analyses were performed for non-TRS and TRS polygenic risk scores with an unadjusted statistical threshold of p < 0.05. Additional post-hoc analyses were conducted for TRS polygenic risk that also included non-TRS polygenic risk score in the model in order to confirm TRS results as independent of non-TRS effects. Because of the directional nature of hypotheses (i.e., greater presynaptic dopamine synthesis capacity (Ki) expected with greater non-TRS risk and less TRS risk), one-tailed p-values are provided for each test.
Post-hoc voxelwise general linear model analyses of Ki values to more finely localize results within the striatum were conducted with SPM software (https://www.fil.ion.ucl.ac.uk/spm/software/) using a one-tailed, voxel-wise threshold of p < 0.005, uncorrected. Models included nuisance covariates for age, sex, and, for genomic analyses, population stratification. Multiple comparisons corrected, threshold-free cluster enhancement (TFCE) statistics were calculated for these models with the TFCE toolbox for SPM (https://neuro-jena.github.io/software.html/; 10000 permutations, Smith permutation method, E = 0.5/H = 2 weighting).
Secondary analyses of [18F]-fallypride data proceeded similarly, with BPND for the thalamus in addition to striatum as outcome variables. Because published data on TRS do not strongly support directional hypotheses for this ligand two-tailed tests were applied to assess the hypothesis that genetic risk may be associated with D2/3 dopamine receptor availability. Following hypotheses-guided regional analyses, exploratory whole-brain voxelwise analyses of [18F]-fallypride data were additionally conducted with a statistical threshold of pTFCE-FWE < 0.05.


留言 (0)