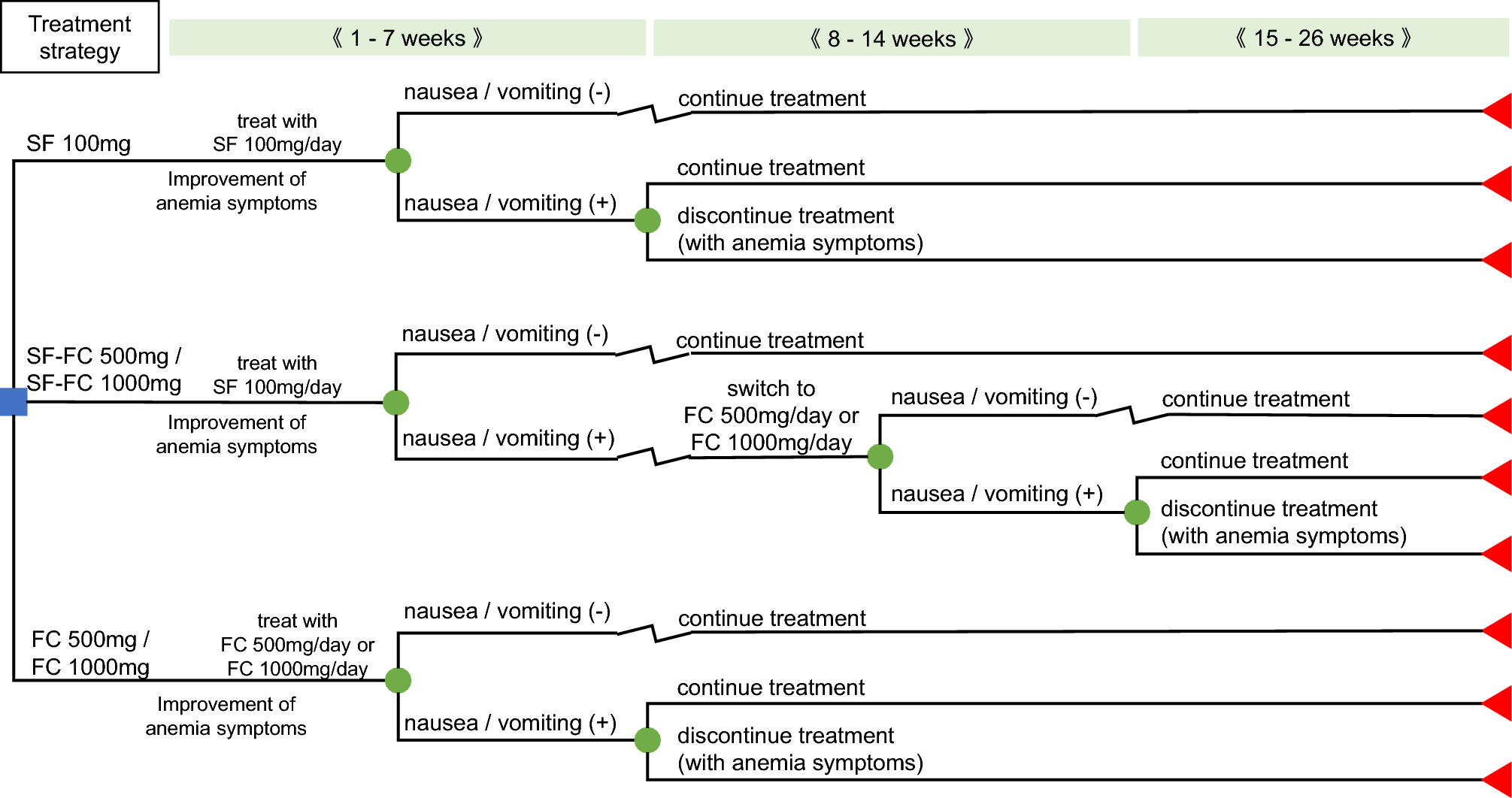
In the present study, we compared the cost-effectiveness of four FC treatment strategies to that of the conventional treatment with SF at 100 mg and evaluated the health economical utility of FC. In all four FC treatment strategies, incremental QALYs were noted relative to SF at 100 mg. The ICER of the SF–FC 500 mg and SF–FC 1000 mg strategies, in which only patients who develop SF-induced nausea/vomiting were switched to FC 500 mg or FC 1000 mg, was lower than JPY 5 million/QALY in the analyses from the Japanese public healthcare payer’s perspective, which was favorable. In the analyses that considered productivity loss from limited societal perspectives, a cost reduction (dominant: the QOL is greater than that of the control and the cost is lower) was found in addition to an improvement in QOL in all four FC treatment strategies. In a comparison with a scenario in which treatment with SF was continued from health economical perspectives, these strategies were considered to be potent treatment options. On the other hand, strategies to initiate IDA treatment with FC at 500 or 1000 mg exceeded JPY 5 million/QALY in the analyses from the Japanese public healthcare payer’s perspective. Although the strategies improved patients’ QOL, patients used FC 500 mg or FC 1000 mg from the beginning regardless of the presence or absence of SF-induced nausea/vomiting, resulting in higher costs. However, cost reduction in addition to improvement in QOL (dominant) were found in the productivity loss-considered analyses from limited societal perspectives in those strategies.
Among the four FC treatment strategies, the drug-switching strategies from SF to FC (SF-FC 500 mg and SF-FC 1000 mg) showed the highest QALYs gained. This may have been because patients who developed SF-induced nausea/vomiting in the drug-switching strategies had the highest rate of patients in whom treatment for IDA could be continued in the 26-week analysis period. Since the discontinuation of treatment for IDA reduces QOL through the symptoms of anemia, QALYs gained may be maximized by inhibiting the rate of patients in whom treatment for IDA is discontinued. This result suggests the importance of continuous treatment for IDA to maintain QOL in patients with IDA.
Conventional oral iron preparations are generally regarded as adequate for the treatment of IDA; however, they may be associated with gastrointestinal adverse events, including nausea, vomiting, abdominal pain, and constipation, which can lead to treatment discontinuation [7, 11, 12]. Another option for IDA treatment is intravenous iron preparations; however, this treatment is highly invasive and adverse events, such as allergic reactions and hypersensitivity, may occur. In addition, time is required for hospital visits, which is not convenient for patients [26]. Therefore, there is a need for an oral iron preparation with fewer gastrointestinal adverse events, which may increase treatment adherence. FC, which has a lower incidence of gastrointestinal adverse events than conventional oral iron preparations, is expected to enable patients to continue treatment for IDA.
Nausea/vomiting related to iron preparations affect QOL and work productivity [9, 10]. Females aged 30–49 years account for the largest percentage of patients with IDA in Japan. Many women of this age are engaged in work and housekeeping/child rearing [27]. As this cost-effectiveness analyses included female IDA patients with a mean age of 40.7 years, the cost reductions could have been more clearly observed in all four FC treatment strategies that have a low risk of nausea/vomiting in the productivity loss-considered analyses from limited societal perspectives.
Within the four FC treatment strategies, QALYs gained and cost-effectiveness were favorable in the drug-switching strategies from SF to FC in the 26-week analysis period. However, when the analysis period was 14 weeks and analyses were conducted from limited societal perspectives, cost reductions in all four FC treatment strategies were maintained. With a shorter treatment period, incremental QALYs of treatment initiated with FC at 500 or 1000 mg, which have a low incidence of nausea/vomiting, were higher than those of the drug-switching strategies from SF to FC. When short-term treatment for IDA is needed or performed, first-line therapy with FC at 500 or 1000 mg may be a treatment option for patients requesting the earlier alleviation of effects on QOL or work productivity. In patients with IDA, treatment needs to be selected in accordance with better QOL, lower productivity loss and individual patient needs for treatment.
In these analyses, we considered work productivity loss with respect to the presence or absence of nausea/vomiting, but not the effects of anemia symptoms. In the present model, compared with FC, SF has higher proportion of patients discontinuing taking iron preparations and the anemia symptom is not ameliorated when discontinuing taking iron preparations, and therefore, work productivity loss due to lack of ameliorating of anemia symptoms in SF is assumed to be greater than in FC. Since productivity loss related to anemia symptoms was not considered in this study, cost reductions by treatment strategies initiating with FC may have been underestimated. IDA is reportedly associated with economic impairments because of physical productivity loss; therefore, the discontinuation of treatment for IDA may result in continuous anemia symptoms, leading to work productivity loss [28]. The four treatment strategies using FC may increase adherence by reducing the risk of oral iron preparation-induced gastrointestinal adverse events such as nausea/vomiting. As a result, the number of patients with attenuation of anemia symptoms may increase compared to that of patients with SF.
This study has a number of limitations that need to be addressed. First, although the patients gradually adapted, experiencing relief of symptoms of nausea/vomiting in the continuation of treatment, the present model assumes that nausea/vomiting continuously occurred for 9.7 days per 7 weeks until treatment switching or discontinuation. However, the results of the 14-week analyses were similar to those of the 26-week analysis; therefore, the effect on the results obtained herein may be weak. Second, there may be a specific number of patients in whom treatment with iron preparations did not improve the symptoms of anemia in actual clinical practice; however, we assumed that symptoms of anemia may be ameliorated with all the patients who continue the treatment with FC or SF in the present model’s structure. On the other hand, the proportion of the patients without improvements would be similar between FC and SF, if such patients did exist. Therefore, its effect on the present results was considered to be negligible. Third, the severity of nausea/vomiting and temporal changes in symptoms are not considered. In the phase III study [13], the severity of nausea/vomiting was evaluated, and all cases were mild or moderate, no severe case was observed. In contrast, the severity of nausea/vomiting was not considered in the present study, because the web-based survey data used to determine disutility could not obtain the values according to the severity of nausea/vomiting [9]. However, since there was no significant difference in the distribution of severity and duration of nausea/vomiting between the FC and SF groups in the phase III study [13], the temporal change in symptoms is assumed to be the same in both groups, the effect on the results obtained herein may be limited. In addition, the impact of disutility of nausea/vomiting was evaluated by deterministic sensitivity analyses (Fig. 2), and the results did not change over the range of the settings.





留言 (0)