DREAMM-11 was a Phase 1, open-label study of belantamab mafodotin monotherapy (Part 1) [11], and combination therapy (Part 2) in patients with RRMM. This was the first study to investigate the tolerability, safety, efficacy and PK of belantamab mafodotin alone and in combination with the SoC regimens bortezomib plus dexamethasone and pomalidomide plus dexamethasone, specifically in a Japanese patient population. In Part 1, both doses of belantamab mafodotin monotherapy were tolerated [11]. Similarly, in Arm A of Part 2, the combination of belantamab mafodotin with bortezomib plus dexamethasone was also tolerated, with no DLTs reported. Hepatoxicity is known to be associated with pomalidomide treatment [13], and, in the four patients who received belantamab mafodotin in combination with pomalidomide plus dexamethasone, one DLT of liver injury was reported 7 days post-first dose; it was not deemed to be serious and resolved after discontinuation of treatment. According to the 3 + 3 study design for assessing tolerability, the occurrence of a DLT in the first three patients of Arm B required enrolment of an additional three patients. However, as only four patients were enrolled in Arm B, it is not possible to draw any firm conclusions on the tolerability of belantamab mafodotin in combination with pomalidomide and dexamethasone. Nevertheless, a comprehensive safety review of available data determined that no safety concerns were specifically expected with this treatment combination in a Japanese patient population. Similar to Part 1, where no new safety signals for belantamab mafodotin monotherapy were identified in Japanese patients compared with Western patients [6, 11, 14], no new safety signals in Japanese patients were identified with the combinations investigated in Part 2 of the study [7, 8]. Furthermore, the safety profile of each combination was consistent with those of the individual agents [13, 15]. All patients experienced non-serious Grade ≥ 3 AEs; the most common of these across the two treatment arms were thrombocytopenia, lymphopenia and decreased neutrophil counts. Only one SAE (COVID-19 – not related to study treatment) was reported across both treatment arms. Corneal events of a maximum of Grade 3 (based on the protocol-defined scale for keratopathy and visual acuity) were reported in all patients; these were managed with dose delays or interruptions, particularly in patients who had a long duration of treatment and did not require treatment withdrawal, and resolved after a median of 127 days in Arm A and 78 days in Arm B.
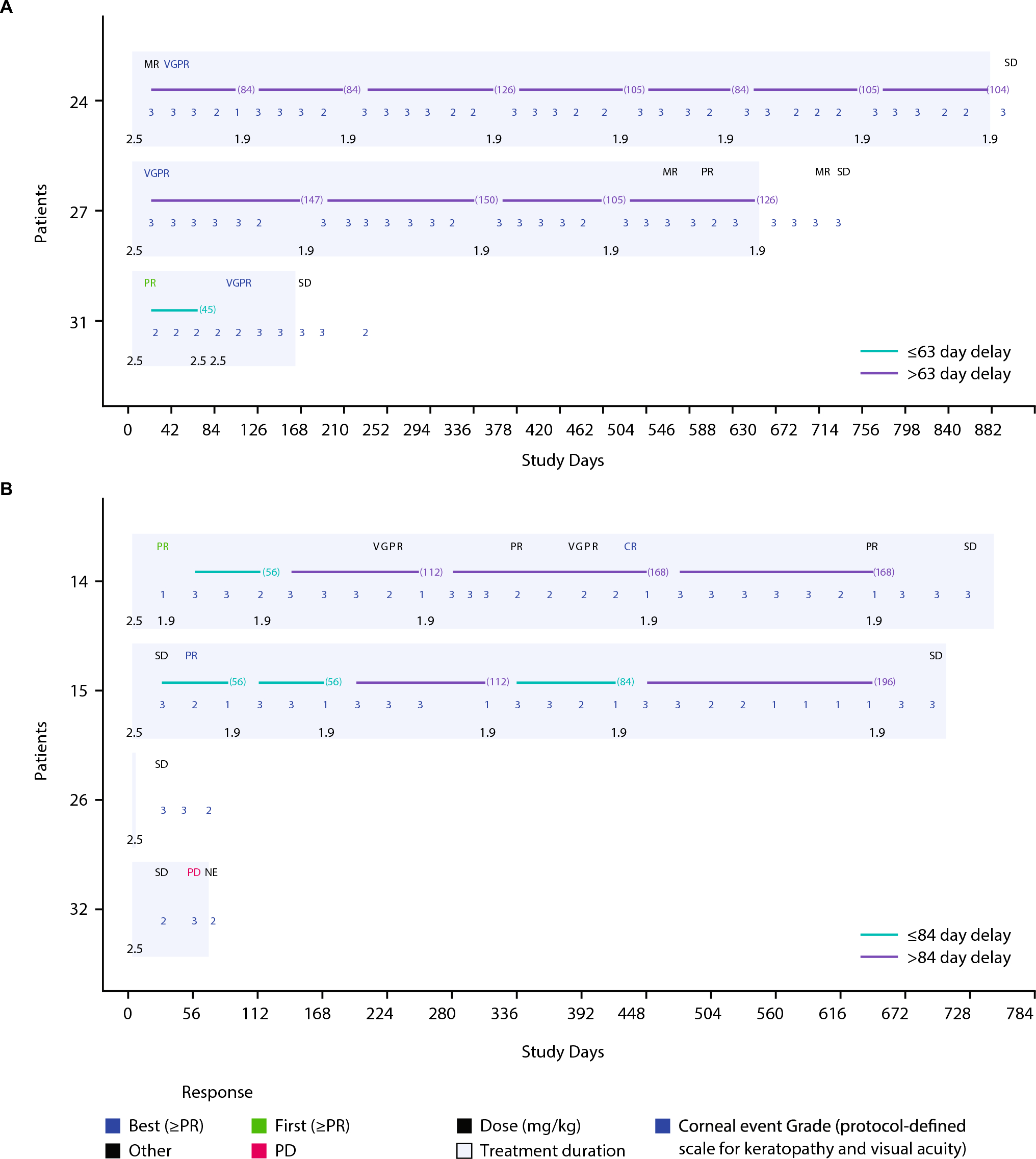
In DREAMM-11 Part 1, ORR with belantamab mafodotin 2.5 mg/kg monotherapy was 50% (2/4 patients) [11]. In Part 2, clinical activity was demonstrated with both combination treatments investigated; all three patients (100%) treated with belantamab mafodotin plus bortezomib and dexamethasone in Arm A achieved an overall response. These findings align with those from the recent DREAMM-7 trial that demonstrated increased PFS, extended time to progression or death, and a clinically meaningful OS trend compared with current SoC (daratumumab plus bortezomib and dexamethasone), in patients with RRMM [7]. All patients in Arm A of the present study demonstrated a deep response (VGPR) to treatment, and two of these responders had a long treatment duration, continuing to receive belantamab mafodotin after the data cut-off date. In Arm B, two of the four patients (50%) treated with belantamab mafodotin plus pomalidomide and dexamethasone achieved an overall response, with one patient achieving a deep response (CR) and the other achieving a PR; both of whom had a long treatment duration. The patient who experienced a DLT during Cycle 1 had stable disease at the time of discontinuation, while the remaining patient withdrew from treatment prior to Cycle 2, due to progressive disease.
Importantly, responses to either of the belantamab mafodotin combination treatments in Arm A and B were sustained despite any dose delays or interruptions. This finding is aligned with the ALGONQUIN study that recently reported an ORR of 89.8% across all doses of belantamab mafodotin in combination with pomalidomide and dexamethasone [8]. Belantamab mafodotin (2.5 mg/kg Q4W for Cycle 1, followed by 1.9 mg/kg for Cycle 2 onwards) in combination with pomalidomide and dexamethasone is also being investigated in the ongoing Phase 3 multicenter trial, DREAMM-8 where ORR was 77% [9]. In DREAMM-8, a statistically significant PFS benefit compared with pomalidomide plus bortezomib and dexamethasone (PVd) as well as a positive trend in OS, and a safety profile that is broadly consistent with the individual agents [9].
While exposure parameters for belantamab mafodotin were slightly higher with the combinations assessed in Part 2 than with belantamab mafodotin monotherapy in Part 1, this was likely due to the small sample size and variability of disease burden between patients in each part of the study. Importantly, PK profiles were as expected based on data obtained for Western patient populations.
A major limitation of the study is the small number of patients included. Nonetheless, Part 2 of this study built on the monotherapy data from Part 1, demonstrating that the combination of belantamab mafodotin with bortezomib/pomalidomide plus dexamethasone led to clinical activity in Japanese patients with RRMM. This study has provided support for the inclusion of Japanese patients in the larger, global, Phase 3 trials of belantamab mafodotin combinations.





留言 (0)