Study design and ethics approval
This manuscript adheres to the Consolidated Standards of Reporting Trials guidelines (Electronic Supplementary Material [ESM] eAppendix).18 This prospective, randomized, parallel-design, open-label, single-centre clinical trial was approved by the ethics committee of Kagoshima University Hospital (Kagoshima, Japan; reference number, 210312). It was conducted from June 2022 to August 2023 at Kagoshima University Hospital. This trial was prospectively registered in a publicly accessible database (UMIN.ac.jp [UMIN000047892]; first posted 30 May 2022). Written informed consent was obtained from all patients before enrolment.
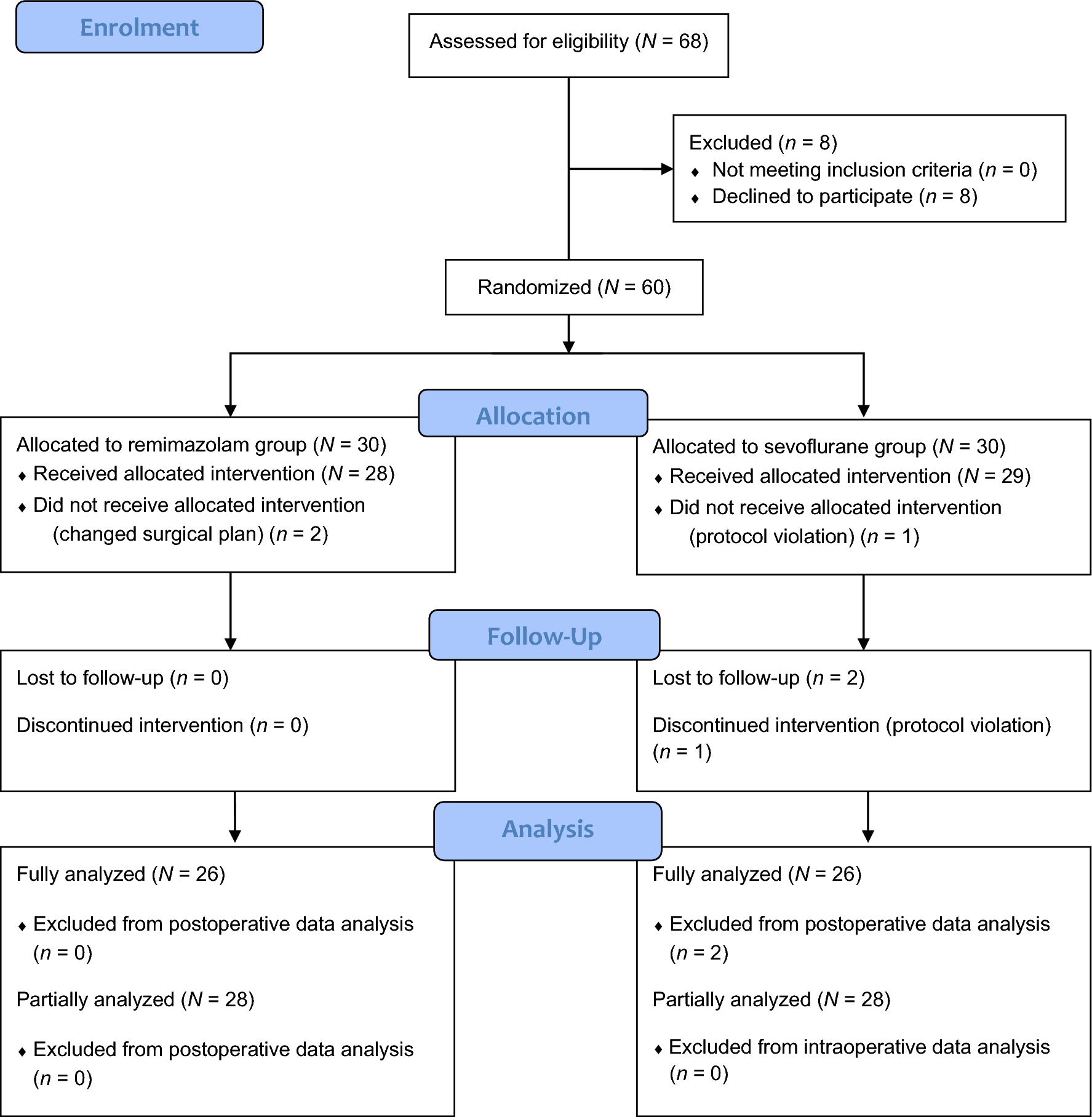
The inclusion criteria were patients with acquired severe aortic stenosis19 (age ≥ 18 yr) undergoing TAVI under general anesthesia. The exclusion criteria were allergy to remimazolam, sevoflurane, midazolam, or flumazenil; a history or family history of malignant hyperthermia; and difficulties in participation because of psychological conditions.
Intraoperative management
The patients were randomly allocated to one of the two groups using internet-based software in a simple randomized manner (Research Randomizer version 4.0).Footnote 1 Patients in the remimazolam group received intravenous remimazolam for maintenance of general anesthesia whereas patients in the sevoflurane group received inhaled sevoflurane. As complete blinding was not possible because sevoflurane administration requires the use of a vaporizer, intraoperative anesthesia care team members were not blinded to group allocation. Two anesthesiologists provided anesthetic management. One anesthesiologist with experience in procedures and perioperative care of patients undergoing TAVI (> 30 patients) supervised anesthesia care and recorded intraoperative variables. Cardiac surgeons and intensivists were responsible for postoperative intensive care. Preoperative patient data were extracted from hospital medical records.
No preoperative sedatives or analgesics were administered in either group. In the operating room, standard perioperative monitoring was initiated per American Society of Anesthesiologists guidelines. The Life Scope J patient monitoring system (Nihon Kohden Corp., Tokyo, Japan) was used to continuously monitor heart rate (HR), direct arterial blood pressure, electrocardiogram, peripheral oxygen saturation measured by pulse oximetry (SpO2), perfusion index (PI) derived from the plethysmographic waveform, end-tidal carbon dioxide tension (EtCO2), and bladder or rectal temperature. The PI was calculated from the pulse oximeter’s infrared signal using the following formula: PI = (pulsatile signal / non-pulsatile signal) × 100. Invasive arterial pressure monitoring was initiated before anesthesia induction. Bispectral Index™ (BIS™) values were monitored using a BIS™ Quatro Sensor (Covidien/Medtronic, Minneapolis, MA, USA). Regional cerebral oxygen saturation (rSO2) was continuously monitored using an INVOS™ 5100C cerebral/somatic oximeter (Covidien/Medtronic).
Intraoperative transesophageal echocardiography was performed after tracheal intubation. A temporary 5-Fr pacemaker wire and a central venous catheter were inserted through the internal jugular vein for rapid ventricular pacing. In the remimazolam group, general anesthesia was induced with remimazolam (6 mg·kg−1·hr−1iv), remifentanil (0.5 μg·kg−1·min−1iv), and rocuronium (0.6–0.9 mg·kg−1iv). The remimazolam infusion rate was reduced to 1 mg·kg−1·hr−1iv after loss of consciousness and adjusted to maintain a BIS of 40–60. In the sevoflurane group, general anesthesia was induced with midazolam (0.05 mg·kg−1iv), remifentanil (0.5 μg·kg−1·min−1iv), and rocuronium (0.6–0.9 mg·kg−1iv). Anesthesia was maintained using sevoflurane (0.5–1.0 age-adjusted minimum alveolar concentration), adjusted to maintain a BIS of 40–60. In both groups, the remifentanil infusion rate was reduced to 0.2 μg·kg−1·min−1iv after tracheal intubation and maintained throughout the TAVI procedure. The infusion rate was adjusted at the attending anesthesiologist’s discretion to ensure adequate analgesia. Considering the high-risk nature of the selected population, remifentanil dose adjustments were permitted for patient safety. The remifentanil infusion rate was reduced to 0.1 μg·kg−1·min−1iv after completing the TAVI procedure. Neuromuscular blockade (train-of-four [TOF] count < 3; TOF-Watch® SX, Organon, Ireland) was maintained with a rocuronium infusion (1–10 μg·kg−1·min−1iv); the infusion was discontinued after valve implantation. Acetaminophen (1 g iv for weight ≥ 50 kg, 0.015 g·kg−1iv for weight < 50 kg) was administered at skin closure. Then, 10 mL of 0.75% ropivacaine was administered via local infiltration. No analgesics other than remifentanil and acetaminophen were used in the operating room. All anesthetic drugs were discontinued after completing postoperative radiography. After confirming a TOF count of > 2, sugammadex (2 mg·kg−1) was administered. In the remimazolam group, flumazenil (0.2 mg iv) was administered immediately after remimazolam discontinuation and was repeated every minute (0.1 mg iv) until the patient responded to verbal stimulation.
In both groups, continuous norepinephrine infusion (0.05–0.08 μg·kg−1·min−1iv) was started when remifentanil started during induction, and it was adjusted to maintain the mean arterial pressure (MAP) at ≥ 60 mm Hg. Intraoperative hypotension (MAP < 60 mm Hg) was treated with a single intravenous bolus of phenylephrine (50–100 μg iv) or ephedrine (4–8 mg iv), depending on the HR. If the HR was < 60 min−1, ephedrine was administered. Other vasopressors or inotropes were used at the discretion of the anesthesia care provider. A colloid bolus (Voluven; Otsuka Pharmaceutical, Tokyo, Japan) of 10 mL·kg−1iv was infused during induction, followed by continuous infusion of a balanced crystalloid (Bicanate; Otsuka Pharmaceutical, Tokyo, Japan) at a rate of 2–8 mL·kg−1·hr−1iv. The attending anesthesiologists were allowed to administer three boluses (30 mL·kg−1iv) of the colloid if needed. Red blood cells were transfused to maintain hemoglobin concentrations of 8–10 g·dL−1. Fresh-frozen plasma or platelets were transfused if blood loss exceeded 1,000 mL and if clinically insufficient hemostasis was suspected by surgeons or anesthesiologists. Vasodilator use was at the discretion of the anesthesia care provider. During anesthesia induction and after cessation of anesthetic drug administration, the lungs were ventilated with an inspired oxygen fraction (FIO2) of 1.0 with a fresh gas flow of 6 L·min−1. After tracheal intubation, the lungs were ventilated with an FIO2 of 0.4 with a fresh gas flow of 3 L·min−1 and a tidal volume (TV) of 6–8 mL·kg−1 of ideal body weight. The respiratory rate was adjusted to maintain an EtCO2 of 35–45 mm Hg and a positive end-expiratory pressure of 5–8 cm H2O. Intraoperative data were recorded every 20 sec. The patients were warmed using a forced-air warming system (Cocoon™ Connective Warming System, Care Essentials Pty Ltd., North Geelong, VIC, Australia) to maintain normal core temperature.
Primary and secondary outcomes
The primary outcome was time to extubation, defined as the time from cessation of remimazolam or sevoflurane administration to extubation. The extubation criteria were eye opening with verbal stimulation, presence of spontaneous ventilation with a TV of > 5 mL·kg−1 of ideal body weight and a respiratory rate of 10–20 min−1, hemodynamic stability (MAP of 60–140 mm Hg and HR of 50–120 min−1), and recovery of TOF ratio to > 1.0. The patients were verbally stimulated every 20 sec after anesthetic drugs were discontinued.
The secondary outcomes were MAP, HR, SpO2, PI, rSO2, BIS, and core body temperature during general anesthesia; vasopressor doses during general anesthesia; and intra- and postoperative complication rates, as defined by the Valve Academic Research Consortium 3 (VARC-3).20 We compared intraoperative variables at seven timepoints: baseline (before induction), 120 sec after tracheal intubation, 30 sec before the start of the operation, 30 sec before valve implantation, minimal values during valve implantation (except HR), 30 sec before the end of the operation, and 120 sec after extubation.
Intra- and postoperative complications
Intraoperative complications included conversion to open surgery, unplanned use of mechanical circulatory support, valve malpositioning, and severe paravalvular regurgitation. The patients were followed up for 30 days postoperatively. Postoperative data were obtained from hospital medical records. The extracted postoperative complications were length of stay in the intensive care unit (ICU), length of stay in the hospital, postoperative nausea and vomiting (PONV), neurologic events (stroke and delirium), hospitalization (except for pre-existing conditions), bleeding (overt bleeding that required a transfusion of 1 unit of whole blood/red blood cells), vascular/access-related complications, cardiac structural complications (cardiac structure perforation/injury/compromise, new pericardial effusion, or coronary obstruction), new conduction disturbances and arrhythmias, acute kidney injury (meeting at least one of the following criteria: a 150–200% increase in serum creatinine compared with that at baseline, or an increase of > 0.3 mg·dL−1 [26.4 mmol·L−1] within 48 hr of the index procedure), myocardial infarction (requiring treatment), bioprosthetic valve dysfunction (including nonstructural valve dysfunction, thrombosis, and endocarditis), leaflet thickening and reduced motion, clinically significant valve thrombosis, technical success at exit from operating room, device success at 30 days, and all-cause mortality at 30 days. The aortic valve area, aortic regurgitation, and mean aortic valve pressure gradient were also extracted from hospital medical records.
Intensive care unit admission and management was determined at the discretion of cardiac surgeons and intensivists. Postoperative nausea and vomiting and delirium were recorded at least twice daily in the ICU. Attending ICU nurses recorded delirium using the Confusion Assessment Method for the ICU.21
Statistical analysis
Categorical data are presented as absolute and relative frequencies. Group comparisons were performed using the Chi square or Fisher’s exact test depending on the expected cell counts of corresponding contingency tables. Continuous data are presented as mean and standard deviation (SD) or median and interquartile range [IQR], depending on the distribution. The unpaired t test or Mann–Whitney U test was performed to assess differences between groups. Differences in medians and their 95% confidence intervals (CIs) were calculated using the Hodges–Lehmann method. We analyzed the time course of intraoperative variables using a mixed model. This model uses a compound symmetry covariance matrix and is fitted using restricted maximum likelihood. In the absence of missing values, this method provides the same P values and multiple comparisons tests as repeated-measures two-way analysis of variance, followed by Sidak’s multiple comparison test. We conducted additional analysis to examine the time course of MAP, HR, PI, and rSO2 by adjusting for baseline values. The values at each timepoint were normalized by dividing them by the baseline values. All statistical tests were performed with a two-sided 5% significance level. Statistical analyses were performed using Prism version 10.2.3 (GraphPad Software, San Diego, CA, USA). More precisely, it is a modified version of R commander designed to add statistical functions frequently used in biostatistics.22
One of the most important complications after TAVI is stroke (reported incidence, 2–4%), which is associated with adverse outcomes.7,8 Further, more than half of perioperative strokes occur within 24 hr after TAVI.23 The American Heart Association and American Stroke Association recommend that a stroke alert should be initiated within 5 min from symptom discovery.9 We thus determined that a 5-min difference in time to extubation was clinically important to minimize permanent neurologic dysfunction after stroke. To detect a 5-min difference in time to extubation with a two-sided approximation while accepting an α error of 5% and a β error of 20%, we calculated the required study size as 48 patients based on preliminary data using Power and Sample Size Calculation version 3.1.2 (Dupont WD and Plummer WD, Vanderbilt University, Nashville, TN, USA). Preliminary data were calculated from patients who underwent TAVI at our institution (number of patients, 20; mean [SD] time to extubation, 12 [6] min). To account for patient dropout, we added 25% more patients, resulting in a final sample size of 60 patients.



留言 (0)