
記住我


We analyzed all adult ICU admissions for COVID-19 in Ontario between 1 March 2020 and 31 July 2021, and identified 72 hospital corporations with at least one adult COVID-19 ICU admission. Of these, 58 (80%) were CHCs and 15 (20%) were AHCs (Table 1). At baseline, these corporations had 1,820 adult ICU beds: 1,002 (55.1%) in CHCs and 818 (44.9%) in AHCs. Community hospital corporations had a median [IQR] of 10 [5–35] adult ICU beds at baseline, while AHCs had a median [IQR] of 36 [24.5–83] adult ICU beds. These numbers did not include additional ICU beds that may have been added during the pandemic.
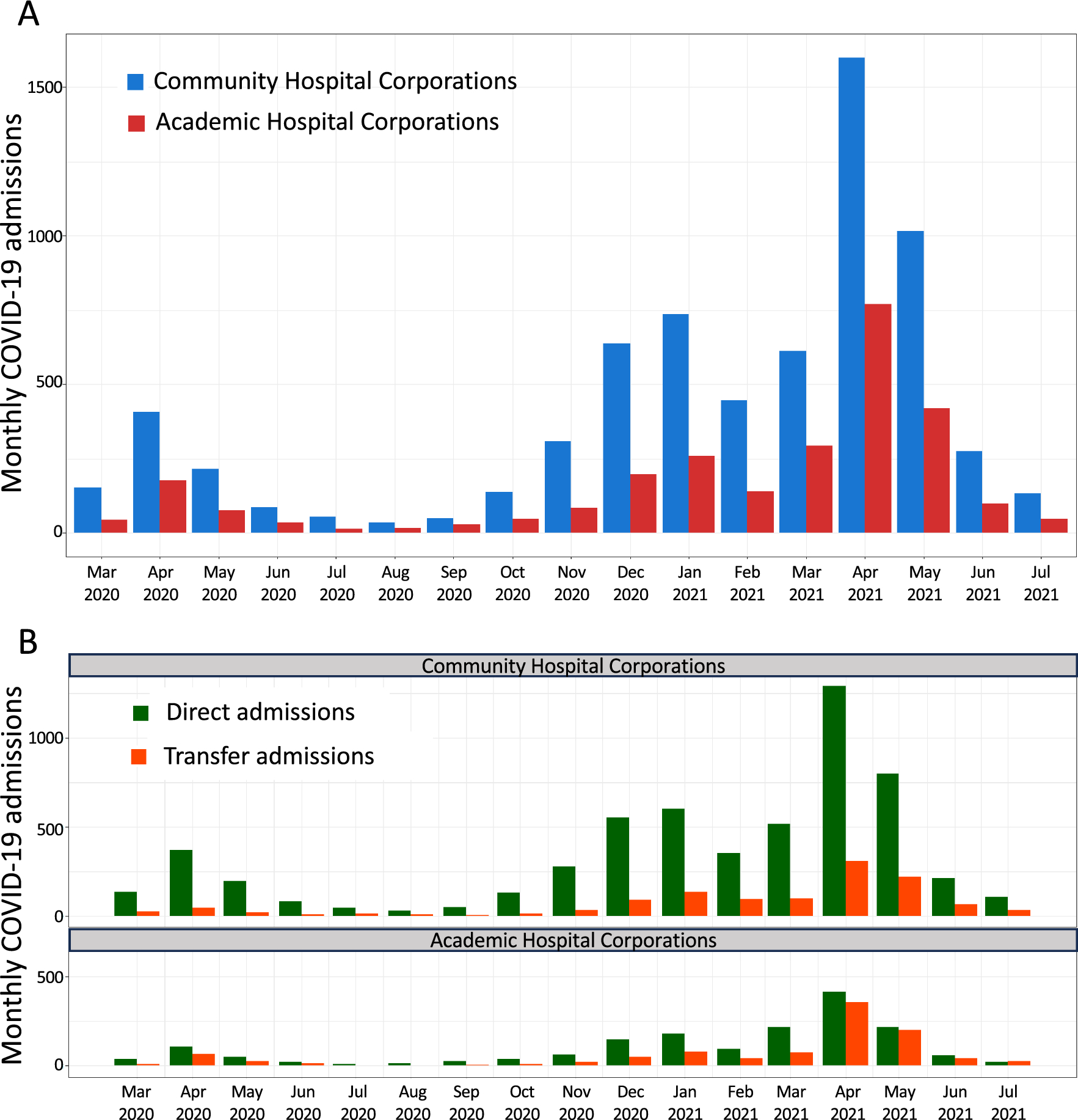
Table 1 Number of hospital corporations and baseline intensive care unit beds in community and academic hospital corporations in Ontario, CanadaBetween 1 March 2020 and 31 July 2021, there were 9,651 adult ICU admissions for COVID-19 in Ontario: 6,902 (71.5%) in CHCs and 2,749 (28.5%) in AHCs, corresponding to 6.9 (95% CI, 6.7 to 7.1) admissions per baseline ICU bed in CHCs and 3.4 (95% CI, 3.2 to 3.5) in AHCs (P < 0.001) (Table 2). Intensive care unit admissions varied between peak and trough periods, but the percentage of admissions in CHCs was consistently 60–80% (Fig. 1A). Two different types of ICU admissions were reported: “direct” admissions, originating from within the same hospital corporation, such as the emergency department or ward, and “transfer” admissions, originating from another hospital corporation. Direct admissions were more common than transfer admissions in both CHCs and AHCs; however, the percentage of transfer admissions in AHCs increased during peak periods, reaching nearly 50% in April 2021 (Fig. 1B).
Table 2 Adult COVID-19 intensive care unit admissions and intensive care unit days of COVID-19 care provided in community and academic intensive care unitsFig. 1
Adult COVID-19 admissions in community hospital corporations and academic hospital corporations during the first three waves of the pandemic. (A) Monthly COVID-19 ICU admissions in CHCs and AHCs. Blue bars: CHC admissions. Red bars: AHC admissions. (B) Monthly direct admissions and transfer admissions in CHCs and AHCs. Green bars: direct admissions. Orange bars: transfer admissions.
AHC = academic hospital corporation; CHC = community hospital corporation; ICU = intensive care unit
There were 131,838 days of ICU care (ICU days) provided to adult patients with COVID-19 in Ontario. Of these, CHCs provided 88,571 (67.2%) ICU days and AHCs provided 43,267 (32.8%) ICU days, corresponding to 88.4 (95% CI, 87.8 to 89.0) ICU days per baseline ICU bed in CHCs and 52.9 (95% CI, 52.4 to 53.4) ICU days per baseline ICU bed in AHCs (P < 0.001) (Table 2).
Burden of COVID-19 intensive care unit care in individual hospital corporationsIndividual hospital corporations provided from < 100 ICU days to > 10,000 ICU days of COVID-19 care (data not shown). As a result of this heterogeneity, 18/72 (25%) hospital corporations (11 CHCs and seven AHCs) provided > 70% of ICU COVID-19 care in the province. There was also significant variation in the number of ICU days of COVID-19 care relative to baseline ICU beds. Figure 2 shows the 20 hospital corporations with the highest number of ICU days per baseline ICU bed while Electronic Supplementary Material (ESM) eFigure shows all Ontario hospital corporations having at least one baseline adult ICU bed.
Fig. 2
Intensive care unit days of adult COVID-19 care per baseline intensive care unit bed. Shown are the 20 hospitals with the highest number of ICU days per baseline ICU bed. Blue: community hospital corporations. Red: academic hospital corporations.
ICU = intensive care unit
Notably, CHCs had both the highest and lowest number of patients with COVID-19 per baseline ICU bed. We therefore compared high and low occupancy CHCs with respect to baseline ICU bed numbers and noted that high occupancy CHCs had a higher mean (SD) number of baseline ICU beds than low occupancy CHCs (28 [21] vs 8 [4] beds; P < 0.001). We therefore subdivided CHCs into “large” and “small,” based on the median number of baseline ICU beds. Large CHCs, with > 10 beds, provided a significantly higher median [IQR] number of ICU days of COVID-19 care per baseline ICU bed than both AHCs and small CHCs (73.7 [53.8–110.6] vs 42.2 [32.7–71.8] vs 21.4 [7.2–40.3] ICU days; P < 0.001) (Fig. 3).
Fig. 3
Intensive care unit days of adult COVID-19 care per baseline intensive care unit bed, by hospital type. Shown are the top 20 hospital corporations.
CHC = community hospital corporation; AHC = academic hospital corporation; large CHC ≥ 10 baseline ICU beds; small CHC ≤ 10 baseline ICU beds; ICU = intensive care unit
Patient characteristicsUsing patient-level data, we compared the demographic and clinical characteristics of ICU patients with COVID-19 in CHCs and AHCs (Table 2). We first compared patients who were directly admitted, i.e., those admitted to the ICU from within the same hospital corporation. Out of 7,306 direct ICU admissions, 5,619 (76.9%) were in CHCs and 1,687 (23.1%) in AHCs (Table 3). Direct admissions to CHCs had higher mean (SD) MOD scores on admission (4.2 [2.6] vs 3.9 [2.6]; P < 0.001) and lower ratios of arterial oxygen partial pressure to fractional inspired oxygen concentration (P/F ratio) [189 (176) vs 267 (221); P < 0.001], indicating more severe hypoxemia. In addition, they were invasively ventilated on more days (47.4% vs 40.9% of ICU days; P < 0.001) and noninvasively ventilated on more days (25.0% vs 17.7% of ICU days; P < 0.001) (Table 3). Use of renal replacement therapy was similar. ECMO, which is only available in a small number of AHCs, was used more frequently in AHC direct admissions (1.2% vs 0.1% of ICU days; P < 0.001) and the median [IQR] ICU length of stay was also slightly longer among AHC patients (7.3 [3.4–16.6] days vs 7.0 [3.2–14.5] days; P = 0.02).
Table 3 Characteristics of “direct” admission patients in community hospital corporations and academic hospital corporationsWe next analyzed transfer ICU admissions, i.e., patients admitted to the ICU from another hospital corporation, often as a second ICU admission. Patients with transfer admissions in AHCs were younger than those in CHCs (55.6 vs 62.6 yr; P < 0.01) (Table 4). The mean (SD) MOD scores on admission were higher (6.3 [2.7] vs 5.6 [2.9]; P < 0.01) and mean (SD) P/F ratios were lower (217 [183] vs 235 [184]; P < 0.001). In addition, transfer patients in AHCs were invasively ventilated on more days (80.3% vs 69.0% of ICU days; P < 0.01) although noninvasively ventilated on fewer days (3.9% vs 10.2% of ICU days; P < 0.01). Extracorporeal membrane oxygenation was significantly more common among AHC patients (12.5% vs 0.02% of ICU days; P < 0.001) and the median [IQR] ICU length of stay was also longer (13.3 [6.2–25.1] days vs 10.8 [5.0–21.5] days; P < 0.001).
Table 4 Characteristics of “transfer” admission patients in community hospital corporations and academic hospital corporationsDischarge destinationsDischarge destinations were classified into four categories: 1) discharge from the ICU, 2) transfer to another ICU, 3) deceased/palliative, and 4) other (ESM eTable). Discharge from the ICU was more common among AHC patients (55.3% vs 51.6%; P = 0.002) while transfer to another ICU was more common among CHC patients (21.0% vs 16.1%; P < 0.001) (Table 5). The percentage of patients who were deceased/palliative was similar in CHCs and AHCs (27.0% vs 28.2%; P = 0.26); however, this did not account for the final outcomes of patients who were transferred to other ICUs on discharge.
Table 5 Discharge destinations for patients admitted to community and academic intensive care unitsMortalityTo account for patients who were transferred between ICUs, we used birthdate, sex, and date of transfer to match admission records corresponding to a single illness episode. This changed the discharge destination for 733 patients. Table 6 shows patient discharge destinations based on index hospital (hospital of first admission). Discharge from the ICU was more common among AHC patients (59.2% vs 56.3%; P = 0.01) while transfer to another ICU was equally common among CHC and AHC patients. Deceased/palliative was more common among CHC patients (30.4% vs 27.5%; P = 0.009).
Table 6 Discharge destination for patients with index admission to a community or academic intensive care unitWe applied logistic regression to model the odds ratio (OR) for death based on index admission to a CHC or AHC. In a univariable model, the OR for mortality was lower for AHC patients (OR, 0.87; 95% CI, 0.78 to 0.97; P < 0.001) (Table 7). Nevertheless, in a multivariable model that included age, sex, and severity of illness at first ICU admission (MOD score), the adjusted OR for mortality was similar for AHC and CHC patients (Table 7).
Table 7 Univariable and multivariable logistic regression models for mortality based on index hospital typeExtracorporeal membrane oxygenation therapyExtracorporeal membrane oxygenation is the most advanced therapy for patients with severe acute respiratory failure. In Ontario, it is only available in a small number of AHCs, so most patients are transferred to receive ECMO. We modelled the likelihood of receiving ECMO based on index hospital type. In a univariable model, the OR for ECMO was significantly higher among patients whose index admission was in an AHC (OR, 6.62; 95% CI, 5.10 to 8.67; P < 0.001) (Table 8). This effect persisted in a multivariable model that included age, sex, and severity of illness at first ICU admission (MOD score) (adjusted OR, 6.16; 95% CI, 4.72 to 8.11; P < 0.001).
Table 8 Univariable and multivariable logistic regression models for the likelihood of receiving extracorporeal membrane oxygenation
留言 (0)