Here, we provide a framework for teaching MR on inpatient rounds during discrete moments of a patient’s hospital stay: admission, ongoing uncertainty, and discharge. This framework integrates the aforementioned teaching tools,6,7,8 with the underlying theories and clinical principles that support their use.17,18,19,20,21,22
Apply Management Scripts on Admission
While clinical cases have varying degrees of diagnostic uncertainty (for which we refer readers to strategies for teaching DR on rounds16), there is often reasonable clarity around a working diagnosis, which can allow for the prioritization of management decisions during oral presentations and rounding conversations.9 Clinical teachers can promote learners’ development and application of MR during new patient presentations by routinizing the explicit use of the management script template.6,7,8
The management script template offers a structured approach to organizing and articulating MR on rounds.6,7,8 Described previously, a management script4,6,17,23 is a mental file of specific management strategies that clinicians activate and apply within a given context. During inpatient rounds, clinicians first activate a management script, which includes many illness-specific interventions, not all of which may be necessary or relevant in a given case, and then select from multiple management options to enact a plan.6 The management script template6,7,8 is a teaching tool that can be used during case presentations on rounds to explicitly consider these two steps, management script activation and option selection, in the context of a given clinical case. In our experience, clearly articulating these steps during inpatient rounds allows for a more nuanced discussion of a patient-centered management plan including consideration of risk and benefit for each intervention in the context of the patient’s goals and any system barriers. This discussion should include reasons for not doing many of the options on the initial management script.
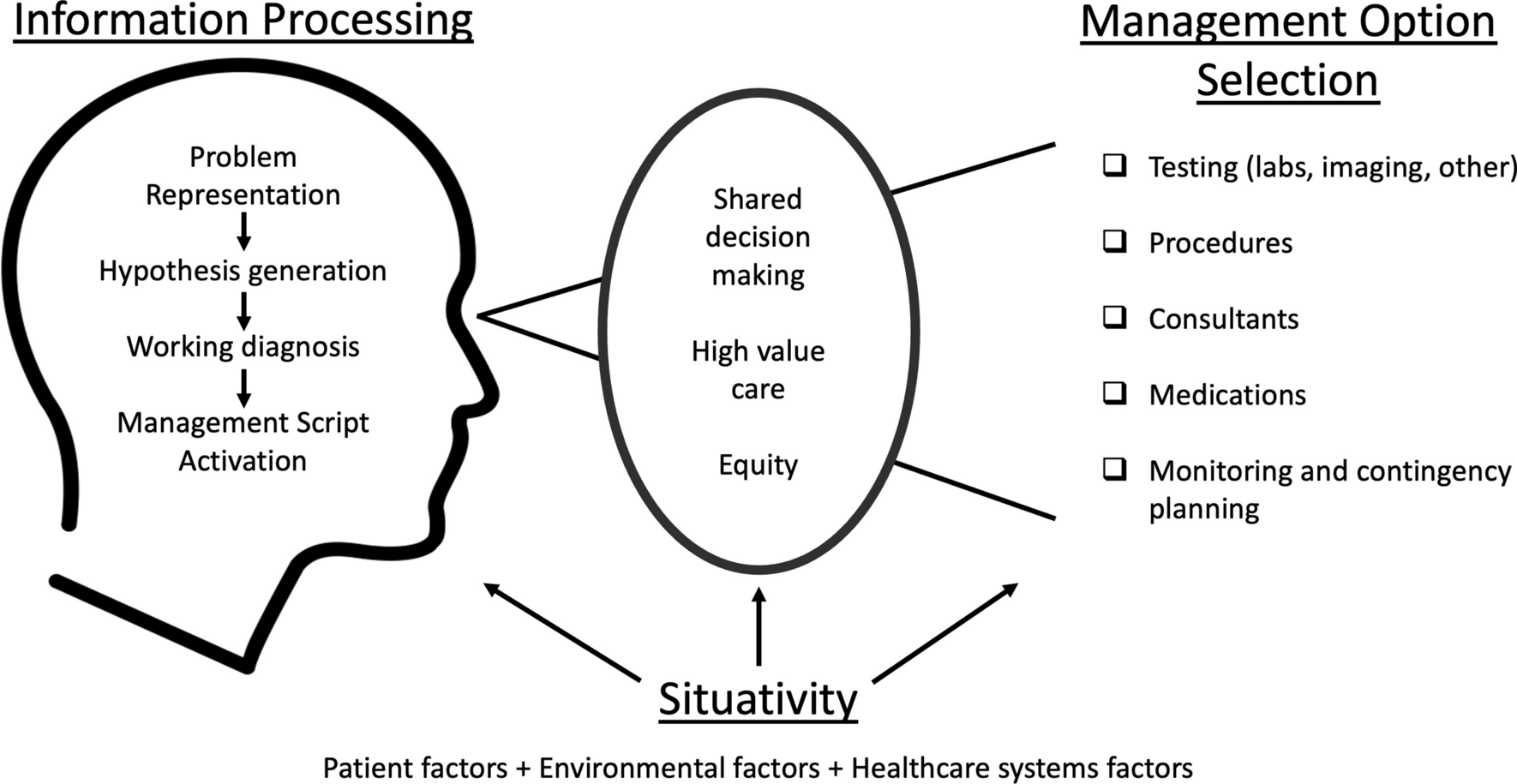
These discrete steps align with IP and situativity theories. In activating a management script, clinicians draw on their stored content knowledge for a specific clinical problem (IP theory). In selecting among multiple options and enacting a management plan, they adapt to contextual factors (situativity theory, see Fig. 1). The accommodation of contextual factors is a more advanced step and requires consideration of shared-decision making, high-value care, and equity, among other clinical principles. Clinical teachers can advance MR instruction on rounds by encouraging learners to elaborate an organized structure for the problem-specific management script they are activating (a task most suitable to early learners still developing their knowledge structures), probing learners to explicitly articulate the content- and context-related factors that influence their management option selection. For more advanced learners, clinical teachers can incorporate counterfactuals and contingency planning (e.g., “What would you do if…”) into case presentations and MR discussions (Table 1, row 2).
Table 1 Application of the Framework for Teaching MR on Inpatient RoundsUse the Management Pause During Moments of Uncertainty
Ideally, enacting an initial management plan for a hospitalized patient would be a relatively straightforward process and lead to a patient’s clinical improvement. However, clinicians may need to contend with uncertainty during inpatient rounds, such as when a patient does not respond as expected to an initial management plan, requiring reconsideration of the working diagnosis and/or the previously established management decisions. The management pause7 offers a practical tool for clinical teachers to promote deliberate engagement with this uncertainty, whether it be their own uncertainty or that of the learners they work with, during authentic case discussions on rounds. The management pause also explicitly centers patient preferences and shared decision-making during these challenging moments of clinical practice.
Initially adapted from the diagnostic pause,24 the management pause slows MR down, prompts intentional consideration of management options, and assures integration of the patients’ perspective.7 This intentional discussion of risks, benefits, and alternatives supports the important engagement of system 2 thinking (i.e., “deliberative mind”25), consistent with IP theory. Effective MR during inpatient rounds, especially in moments of uncertainty, also requires alignment with patients’ values and preferences (e.g., contextual factors), of which clinicians are often unaware.26,27,28,29,30 In helping clinicians incorporate the patient’s perspective into moments of uncertainty, the management pause forces consideration of contextual factors and aligns with evidence that patients prefer direct and explicit discussion of uncertainty.29,30
While the astute clinical teacher can apply the management pause in various educational situations on rounds, we propose moments of uncertainty as a fruitful opportunity for use. In these moments, the management pause can help faculty and trainees alike manage uncertainty by facilitating exploration of proposed management decisions, prompting learners to reflect on clinical and contextual factors influencing their decisions, preparing them for bedside conversations that facilitate the integration of shared decision-making into MR, and helping them collaborate with patients to clarify next steps, contingency plans, and thresholds for adjustment (e.g., “if X happens, we will get Y test or change Z treatment.”).31 Table 1 (row 3) uses the sample UGIB case to apply the management pause to a moment of uncertainty about how to best manage the patient’s anticoagulation.
Engage in an Equity Reflection on Discharge
Systemic and individual factors—including implicit bias in clinical decision-making—propagate healthcare inequities, promote further oppression of marginalized groups, and thus require attention when teaching MR.32,33 Associations between outcomes after hospital discharge and patient’s socioeconomic and housing status, race, and language barriers highlight this transition of care as an opportune moment to consider (in)equity in MR when making discharge and follow-up plans during inpatient rounds.34,35,36
Similar to the management pause, the equity reflection7 equips clinical teachers with questions they can ask learners during discharge case presentations, when care plans, follow-up appointments, and system barriers are a frequent consideration (Table 1, row 4) applies the equity reflection to the sample UGIB case). Through the lens of situativity theories, these questions prompt learners to move beyond preconceived knowledge structures and consider contextual factors during discharge. As a result, they help make explicit the often-implicit ways that healthcare systems and clinicians may promote inequity (e.g., by limiting access to certain medications, enacting follow-up plans that require social or financial resources unavailable to marginalized groups, or failing to provide patient education materials in patients’ primary language). The equity reflection also enables consideration of high-value care by asking learners to consider whether individual decisions are right for this patient at this time in this specific context. In addition, by asking trainees to explore ways to leverage the multidisciplinary team to overcome barriers to providing the standard of care, the equity reflection can support trainees in developing the critical consciousness necessary to deconstruct inequitable systems.7
The originators of the equity reflection developed the tool in hopes that regular use will not only prevent further injustices in clinical practice, but also empower learners to develop reflective skills that enable action (rather than self-blame) when they identify bias in their MR.7,37 Structured support for reflective practice can help learners build the metacognitive capacity to recognize and act on implicit bias37,38 and support their self-monitoring during high-stakes clinical decisions.39,40 Discharge discussions offer an important opportunity to explicitly consider unintentional promotion of inequity by employing this teaching tool.
Finally, using the equity reflection requires a foundation of psychological safety. Teachers can build trust with and among team members by embracing vulnerability (e.g., disclosing one’s own moments of bias and lessons learned) and promoting identity safety on clinical teams. In doing so, they can help establish a learning climate that supports learners as they grapple with the charged emotions and the personal and professional identity tensions that can arise when discussing bias and inequity.37,41,42



留言 (0)