
記住我

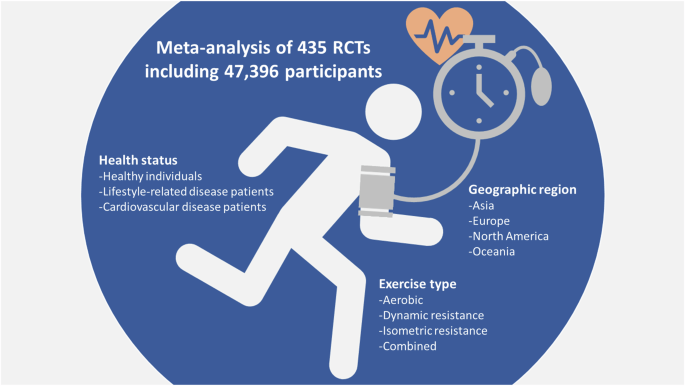

Hypertension is a leading global health issue and a major risk factor for cardiovascular diseases (CVDs); its prevalence is steadily increasing worldwide [1]. Exercise has long been recognized as an effective non-pharmacological intervention for lowering blood pressure (BP), with documented benefits for both healthy individuals and those with lifestyle-related diseases such as hypertension, diabetes, and obesity [2]. However, recent research has highlighted potential variations in the antihypertensive effects of exercise, depending on factors such as the individual’s health status, type of exercise, and even geographic region [3, 4]. The large-scale meta-analysis by Suematsu et al. [5] provides a comprehensive review of the differential impacts of exercise on BP by systematically examining randomized controlled trials (RCTs) to identify how BP responses vary by pathophysiological condition, exercise type, and region (Fig. 1).
Fig. 1
Differential effects of exercise on blood pressure
The meta-analysis by Suematsu et al. included 435 RCTs encompassing 47,396 participants, which allowed a robust exploration of variations in BP response to exercise across different populations [5]. The study found that the effect of exercise on BP varied by health status, with significant BP-lowering effects observed for systolic and diastolic BP in healthy individuals and those with lifestyle-related diseases. Specifically, among patients with lifestyle-related conditions, the average reduction in systolic BP was 5.48 mmHg, while in diastolic BP it was 3.07 mmHg. By contrast, for patients with existing CVDs, exercise did not produce significant BP-lowering effects, with modest reductions in systolic and diastolic BP of 1.16 and 0.46 mmHg, respectively. This difference in BP response highlights the necessity of personalized exercise prescriptions based on health status, especially given the potential risks associated with excessive BP reduction in patients with CVDs.
In addition to pathophysiological differences, Suematsu et al. analyzed the impact of exercise type on BP [5]. Among healthy individuals and those with lifestyle-related diseases, aerobic exercise, dynamic resistance training, and isometric resistance exercise had significant BP-lowering effects. Notably, isometric resistance exercise had the greatest impact in healthy subjects, resulting in systolic and diastolic BP reductions of up to 10.96 and 5.53 mmHg, respectively, compared with other exercise types. However, in individuals with CVDs, most exercise types did not yield significant BP-lowering effects, except for a minor reduction in diastolic BP (1.00 mmHg) associated with isometric resistance training. These findings indicate that isometric resistance exercise, which commonly involves sustained muscle contractions, may be somewhat beneficial for BP management. However, the results suggest that clinicians should proceed with caution when recommending exercise for CVD patients, taking into account the type of exercise as well as its intensity and frequency.
Geographic differences in BP response to exercise were another critical finding of this study, which revealed that BP-lowering effects were not uniform across regions [5]. While BP reduction was significant in most regions, in Oceania, there were limited effects of exercise on systolic and diastolic BP in both healthy individuals and those with lifestyle-related diseases. This outcome could reflect unique regional characteristics, such as dietary habits, physical activity levels, or other lifestyle factors [6] that may influence BP responsiveness to exercise. By contrast, in Asia, significant BP-lowering effects were observed even among CVD patients, which may be linked to region-specific factors such as high salt intake [7]. Suematsu et al. suggest that Asian populations may have heightened sensitivity to BP changes related to salt intake, which may amplify the benefits of exercise on BP management [5]. These regional variations imply that geographic and cultural factors should be considered when generalizing exercise recommendations for BP management.
Suematsu et al.’s study has several notable strengths. First, the inclusion of 435 RCTs provides a substantial dataset, which lends high statistical power to the analysis and enhances the reliability of the findings. Additionally, by exploring BP-lowering effects across various health statuses, exercise types, and geographic regions, the study offers practical insights for developing tailored exercise interventions in clinical settings. The authors’ focus on subgroup differences is particularly valuable, as it underscores the need for personalized approaches to exercise prescriptions rather than a one-size-fits-all recommendation.
Despite these strengths, some limitations are worth noting. One primary limitation is the absence of long-term follow-up data, which restricts the study’s ability to assess the sustainability of BP reductions achieved through exercise. While short-term effects of exercise are well-documented, understanding whether these effects are maintained over months or years is critical for informing long-term BP management strategies. Additionally, the meta-analysis does not account for variations in exercise intensity across the included RCTs, which may influence the results. Consistent reporting of exercise intensity and frequency could enhance the comparability of studies and provide clearer guidelines on the optimal exercise “dose” for BP management.
From a clinical perspective, the findings from Suematsu et al.’s analysis have significant implications for exercise recommendations in high BP treatment. The results suggest that clinicians should consider a patient’s overall health status and specific CVD risks before prescribing exercise as a BP-lowering intervention. For example, in patients with lifestyle-related diseases, aerobic and isometric resistance exercises can be confidently recommended to support BP control. However, in patients with CVDs, careful consideration of exercise type is warranted to avoid potential adverse effects associated with excessive BP reductions. Furthermore, the regional findings indicate that geographic differences, possibly influenced by lifestyle and dietary patterns, should be taken into account. This may mean that population-specific guidelines for exercise and BP management could be beneficial in regions with unique dietary habits, such as the high salt intake in Asia.
Future research should aim to explore the mechanisms underlying these regional differences in exercise response. Studies investigating the interaction between genetic, dietary, and lifestyle factors could clarify why certain populations experience more pronounced BP changes from exercise. Additionally, longer-term studies are needed to evaluate the lasting impact of exercise on BP, particularly in high-risk populations such as those with CVD. Further research could also examine the effects of exercise intensity, as understanding the optimal level of exercise for BP control could lead to more precise recommendations.
In conclusion, Suematsu et al.’s study highlights the varied effects of exercise on BP across different pathophysiological conditions, types of exercise, and regions; these results underscore the need for a personalized approach to exercise prescriptions [5]. The study’s findings provide valuable insights for clinicians, as they suggest that BP-lowering exercise interventions should be carefully tailored to the patient’s health status and, where relevant, geographic region. As the global burden of hypertension continues to rise [1], these insights can inform more effective, individualized exercise guidelines and potentially improve BP management outcomes worldwide.
留言 (0)