
記住我








Hypermagnesemia is a rare complication induced by various causes such as overdosages, increased absorption, and impaired excretion, and therapeutic administration of magnesium-containing drugs is one of the major causes [1]. We report a patient with rectosigmoid cancer with rectal stenosis who developed life-threatening hypermagnesemia due to obstruction of the rectum by fecal masses after preoperative treatment with an oral bowel cleanser containing magnesium citrate solution.
Case presentationWe obtained written informed consent from the patient for the publication of this case report.
A 78-year-old female patient, height 147 cm and weight 47 kg, was scheduled for robot-assisted high-level anterior resection of the colon. She was taking amlodipine for hypertension, magnesium oxide 0.99 g, and sodium picosulfate daily for constipation. Renal function was relatively preserved, with creatinine level of 0.65 mg/dL and eGFR of 65.8 mL/min/1.73 m2. She had an episode which developed dysuria, abdominal pain, and nausea after ingestion of bowel cleaner containing sodium-calcium-ascorbic acid for preparing lower gastrointestinal endoscopy, and had been referred to our hospital with a diagnosis of rectosigmoid cancer. She became restless, complaining of nausea and a sense of weakness following pretreatment with 125 mL of 13.6% magnesium citrate solution and picosulfate sodium hydrate as an oral bowel cleanser 2 days before surgery in our hospital. She developed consciousness disturbance, respiratory depression, and bradycardia in the ward, prompting an in-hospital emergency call on the next day.
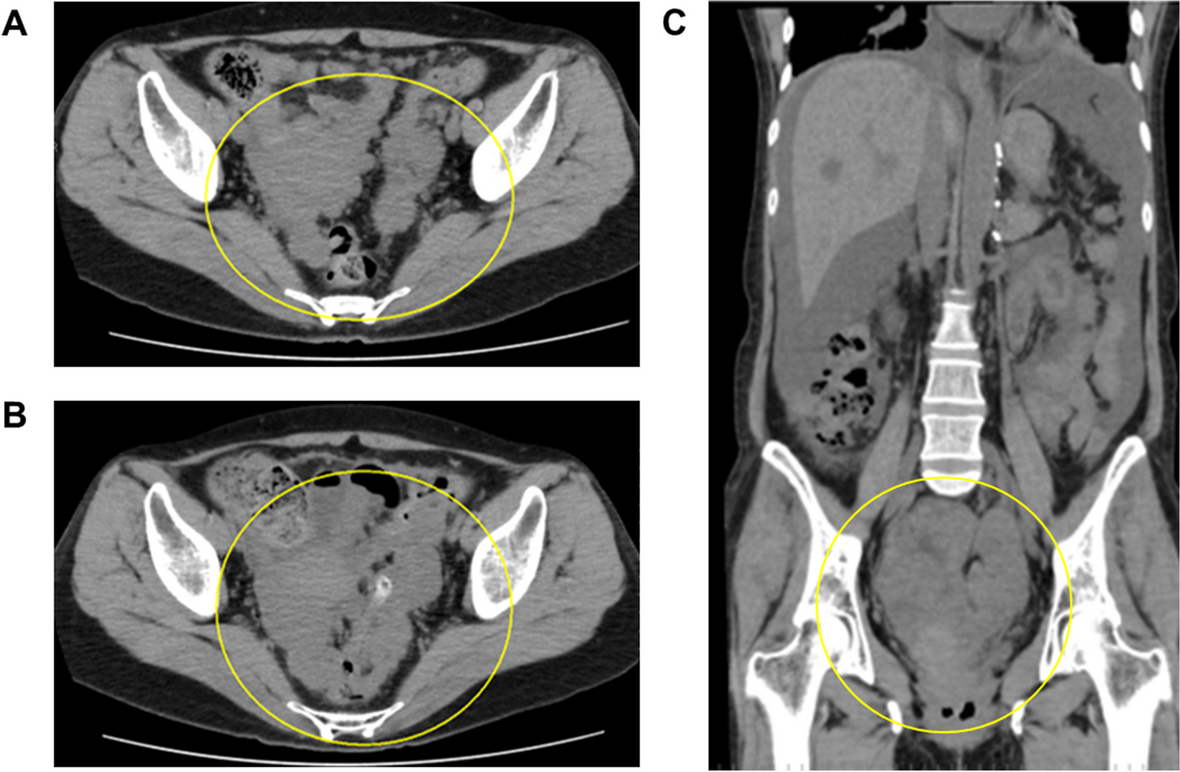
She had SpO2 of 90% under a 10 L/min reservoir mask, sinus bradycardia with a heart rate of 20–30 beats/min, decreased level of consciousness with GCS 3 points (E1V1M1), with isocoric pupils (3.0 mm) but no light reflex. Blood gas analysis showed marked respiratory acidosis: pH 7.023, PaCO2 102 mmHg, PaO2 129 mmHg, HCO3 − 25.2 mmol/L, base excess − 9.0 mmol/L, lactic acid 6.0 mmol/L. Massive regurgitation of the gastric content through the nasal airway was noted, suggesting aspiration pneumonia with carbon dioxide narcosis. The patient was admitted to the ICU with tracheal intubation. A contrast-enhanced CT scan showed a left pleural effusion and collapse of the left lower lobe of the lung, possibly due to aspiration pneumonia, as well as a stenotic lesion in the rectum and dilatation of the colon on the oral side. Head CT showed no intracranial lesions that could decrease the level of consciousness.
The patient frequently exhibited sinus bradycardia and an escape rhythm of premature ventricular contractions, but no ischemic changes in the electrocardiogram (Fig. 1). Transthoracic echocardiography revealed no pericardial effusion and normal left ventricular wall motion. Adrenaline 0.15 μg/kg/min and dobutamine 3 μg/kg/min, along with a rapid infusion of bicarbonate Ringer’s solution, were needed to stabilize her hemodynamics. Blood tests showed normal sodium, potassium, and chlorine levels. Endoscopic examination revealed obstruction of the rectum (Rs) by fecal masses, but no evidence of ischemic or necrotic changes of the colon. As her bradycardia and hypotension improved after endoscopic release of the obstruction, a vagal reflex due to colorectal obstruction seemed to be partly involved in a series of her symptoms, and an emergency Hartmann’s operation was performed.
Fig. 1
Twelve-lead ECG on ICU admission. Ventricular extrasystole, QTc 0.477, and QT prolongation were observed. Sinus bradycardia with a heart rate of 42/min is noted
After surgery, continuous hemodiafiltration was introduced for acute renal failure with serum creatinine of 1.54 mg/dL and KDIGO classification Stage 1, and for metabolic acidosis. The patient’s respiratory and circulatory status remarkably improved, and the tracheal tube was removed on the day after surgery. On postoperative day 1, abnormally high magnesium level of 6.2 mg/dL was noticed, which promoted us to reexamine the stored blood samples. Magnesium levels were 2.6 and 17.5 mg/dL at the time of her admission and emergency call, respectively, suggesting that a series of this patient’s symptoms were due to hypermagnesemia probably caused by the bowel cleanser.
On the second postoperative day, urine output increased and the magnesium level decreased to 3.1 mg/dL with the use of diuretics, so continuous hemodiafiltration was terminated. The patient was discharged from the ICU to the surgical ward on the third postoperative day.
留言 (0)