Patients and study design
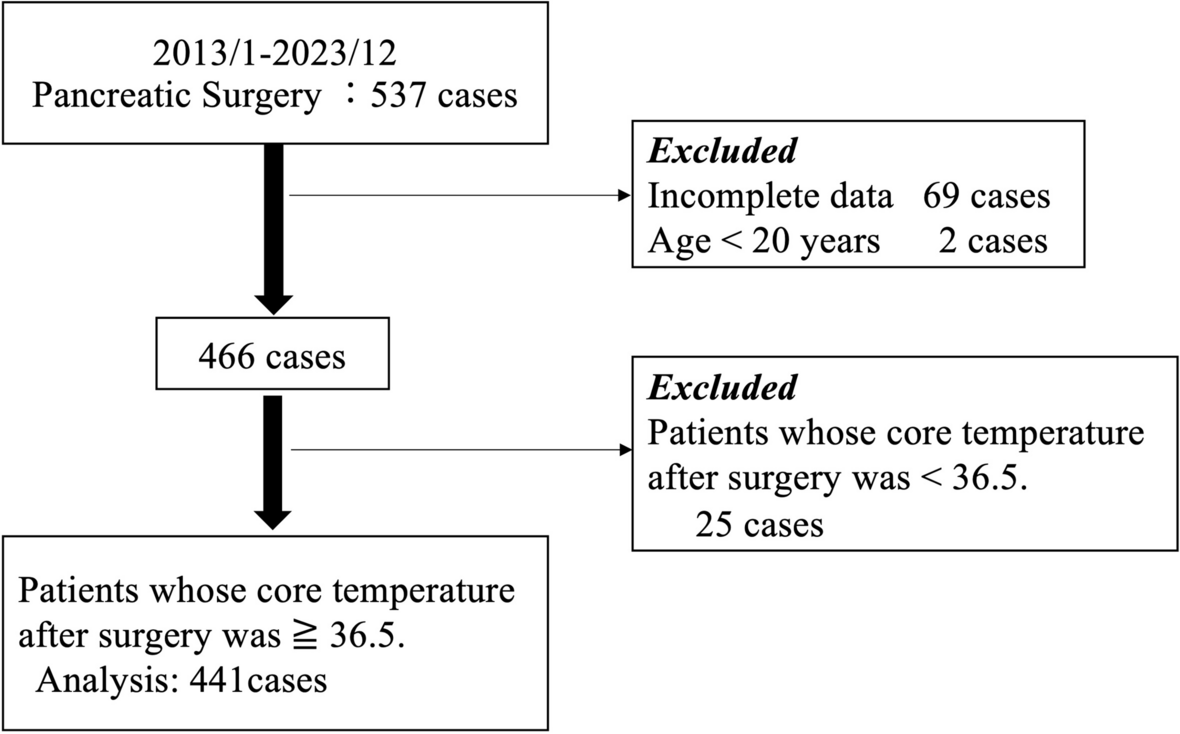
This observational, nonrandomized, retrospective study was approved by the Institutional Clinical Research Ethics Committee of Kyushu University, Fukuoka, Japan (IRB: Clinical Research number #23346–00) and individual written informed consent was waived by the above-mentioned institutional review board. All study protocols were compliant with the Declaration of Helsinki (2013). We enrolled 537 patients who were scheduled to undergo radical surgery for pancreatic cancer at our university hospital between January 2013 and December 2023. Patients with endocrine diseases affecting body temperature, laparoscopic surgery cases, and patients with data defects and under 20 years old were excluded. Data were extracted using a data warehouse (DWH) mining tool (Nihon Kohden, Tokyo, Japan). Data on patient age, body mass index (BMI), operation time, anesthesia time, anesthesia technique (total intravenous anesthesia or volatile anesthesia), administration of flurbiprofen/acetaminophen/pethidine during surgery, amount of bleeding or urine, fentanyl/remifentanil effect site concentration, core temperature, and peripheral (fingertip) temperature were obtained. A shivering incidence was defined as a case of pethidine administration after extubation or a recorded case of shivering as a complication in the electronic anesthesia chart. We regarded muscle activity in more than one muscle as shivering and administrated pethidine for shivering. After insertion of the epidural catheter, anesthesia was induced by the intravenous administration of fentanyl, propofol, and rocuronium, and it was maintained with desflurane (4–5%), sevoflurane (1.5–2%) or propofol (target-controlled infusion of 3–4 µg/mL), remifentanil, and a 40–50% oxygen–air mixture. Additional bolus infusions of fentanyl and rocuronium were administered, as required. To manage postoperative pain, anesthesiologists administered acetaminophen, flurbiprofen, or fentanyl, except for a bolus infusion of epidural anesthesia, before the end of surgery. No opioids were given into epidural anesthesia intra and post-operative period. At the discretion of the anesthesiologist in charge, pethidine was used intra-operatively in a few cases postoperative shivering was expected to occur. Anesthesiologists focused on a target mean blood pressure of 60–70 mmHg during the surgery. For body warming, the double lumen fluid warming system (HOTLINE®, smith medical, Plymouth, MN, USA) and the forced-air warming device (Bair Hugger™ 775 & blanket 522, 3 M, St. Paul, MN, USA) were used for all patients. Warming blanket was covered the upper body at 38–43 ℃ setting, and ambient temperature was set at 26℃ with 40% humidity during surgery and at 28℃ with 50% humidity after surgery.
Statistical analysis
Data are presented as mean (standard deviation) or median (interquartile range) for continuous variables or as percentages for categorical variables. We compared the baseline characteristics between the shivering and non-shivering groups using unpaired t-test, chi-square test, Mann–Whitney U test, or Fisher exact test, as appropriate. Multivariable-logistic regression analysis was performed to estimate the odds ratios (ORs) with 95% confidence intervals (CIs) of postoperative shivering. Variables that did not show a linear relationship with the logit of the outcome were transformed as restricted cubic splines. In the logistic regression, restricted cubic spline with 3 knots located at the 10th, 50th, and 90th percentiles of the variable distribution were used. In the multivariate-adjusted analysis, patient age [7], sex, BMI, operation time, amount of bleeding, postoperative (just after surgery) core and peripheral temperature [10], fentanyl effect site concentration [11], epidural anesthesia [12], anesthesia technique (total intravenous or volatile anesthesia) [13], and administration of flurbiprofen/acetaminophen/pethidine [7, 14, 15] were included in the model to control for confounding factors. These candidates factors have been reported in previous study to be associated with postoperative shivering. The independence of these variables was checked for multicollinearity. Moreover, spline curves were used to visualize the relationship of peripheral temperature, core-peripheral temperature difference, and core temperature with the risk of postoperative shivering. SAS software package (version 9.4; SAS Institute, Cary, NC, USA) was used for all statistical analyses. Two-sided values of p < 0.05 were considered statistically significant in all analyses.









留言 (0)